PULMONARY TUBERCULOSIS
Pulmonary tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis. Robert Koch reported his discovery of the Mycobacterium tuberculosis bacterium in 1882, and its complete genome sequence was mapped over 100 years later. Before COVID-19 pandemic, TB was the most prevalent infectious disease worldwide.
What are the causes of pulmonary TB infection?
People with active TB disease in the lungs or voice box can spread the disease. They release tiny droplets that carry the bacteria through the air. This can happen when they're speaking, singing, laughing, coughing or sneezing. A person can get an infection after inhaling the droplets.
The disease is more likely to spread when people spend a lot of time together in an indoor space, for e.g. living or working together or in a crowded gathering or event.
A person with a latent TB infection cannot pass the disease to other people. A person taking medicine to treat active TB disease usually can't pass the disease after 2 to 3 weeks of treatment. (https://www.mayoclinic.org/diseases-conditions/tuberculosis/symptoms-causes/syc-20351250)
How common is TB?
Not everyone who’s infected with TB gets sick. If you’re infected but have no symptoms, it’s called inactive tuberculosis, or latent TB. TB is dormant (sleeping) inside your body. As many as 13 million people in the U.S. have latent TB. Some people can have a latent TB infection for a lifetime, without ever developing symptoms (active TB).
What are the symptoms of pulmonary TB?
Symptoms of active TB include:
- Bad cough lasting for more than 2 weeks
- Chest pain
- Coughing up blood or sputum
- Fatigue or weakness
- Loss of appetite
- Weight loss
- Chills
- Fever
- Night sweats (https://my.clevelandclinic.org/health/diseases/11301-tuberculosis)
What are the challenges to treat TB infection?
Anti-TB regimens vary depending on the stage and anatomic location of the infection, the immune status and age of the host, the presence of comorbidities, the development of toxicities, drug-drug interactions, and resistance patterns of the bacterium. Resistance of tuberculosis to antibiotics is increasing, and treatment often requires the administration of novel antibiotic combinations that have undergone limited testing in clinical trials. The prolonged duration of therapy needed to eradicate the organism represents an additional challenge. Recently, shorter treatment regimens for latent TB infection have been developed to minimize adverse effects and maximize patient compliance. (https://www.ncbi.nlm.nih.gov/books/NBK441916/)
How is TB infection diagnosed?
History of symptoms along with physical examination of pulmonary system are likely to hint infective pathology. To confirm TB infection, specific tests are required such as:
- Skin test: Site of tuberculin injection is tested for swelling after 48 hours. A positive test indicates you likely have either a latent TB infection or active TB disease. People who had a TB vaccination might get a positive test even if they have no infection.
A negative test means that your body didn't react to the test. It doesn't necessarily mean you don't have an infection.
- Blood test: to find out whether certain immune system cells can "recognize" tuberculosis. A positive test shows that you have either a latent TB infection or active TB disease.
A negative result means you likely do not have a TB infection.
- A chest X-ray can show irregular patches in the lungs that are typical of active TB disease.
- A sputum test in lab can detect the bacteria.
- Breath test, urine test, cerebrospinal fluid test can also be useful in detecting the TB infection. (https://www.mayoclinic.org/diseases-conditions/tuberculosis/diagnosis-treatment/drc-20351256)
How is TB treated?
Active TB treatment
In 2022, the Centre for Disease Control and prevention announced interim guidance on a 4-month anti-TB regimen for drug-susceptible pulmonary tuberculosis. The regimen consists of an intensive phase of 8 weeks of daily Isoniazid (INH), rifapentine, pyrazinamide, and moxifloxacin, followed by a continuation phase of 9 weeks of daily rifapentine, INH, and moxifloxacin.
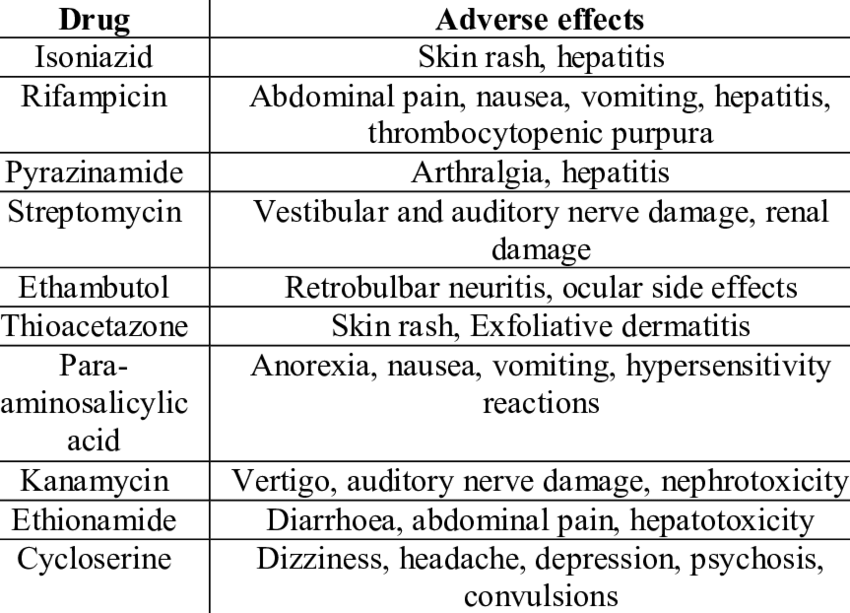
Patients undergoing anti-TB therapy require regular monitoring for clinical response and side effects. Evaluate sputum smears and cultures monthly until 2 consecutive cultures are negative. In patients with chest x-rays and evidence of cavitation who remain culture positive at 2 months, the recommendation is to extend the continuation phase for an additional 3 months (i.e., a total of 9 months of therapy). People who are malnourished, active smokers, immunosuppressed, or with HIV or extensive pulmonary disease may require an extended continuation phase.
Drug-resistant TB
New and repurposed agents include but are not limited to delamanid, bedaquiline, pretomanid, linezolid, amoxicillin-clavulanate, meropenem-clavulanate, imipenem-cilastatin, cotrimoxazole, and macrolides. When prolonged regimens and injectable second-line agents are required, the risks of drug toxicities and patient difficulties with adherence are very high. Interventions to support adherence include psychological counselling and patient education, financial and material incentives, and mobile phone text reminders. New and repurposed agents may permit shorter durations of treatment in some circumstances. Adjuvant surgical excision may be necessary in efforts to eradicate cavities and non-viable lung tissue.
Bacille Calmette-Guerin Vaccine
BCG, a live attenuated strain of M Bovis, has been a WHO-recommended vaccine for infants and children since 1974. This is the most widely used vaccine worldwide, preventing miliary TB and meningitis in infants in countries with high TB incidence. The vaccine is somewhat protective when administered to infants and children, but the protection wanes over several years. (https://www.ncbi.nlm.nih.gov/books/NBK441916/)