Pneumothorax: Causes, Symptoms, Diagnosis, and Treatment
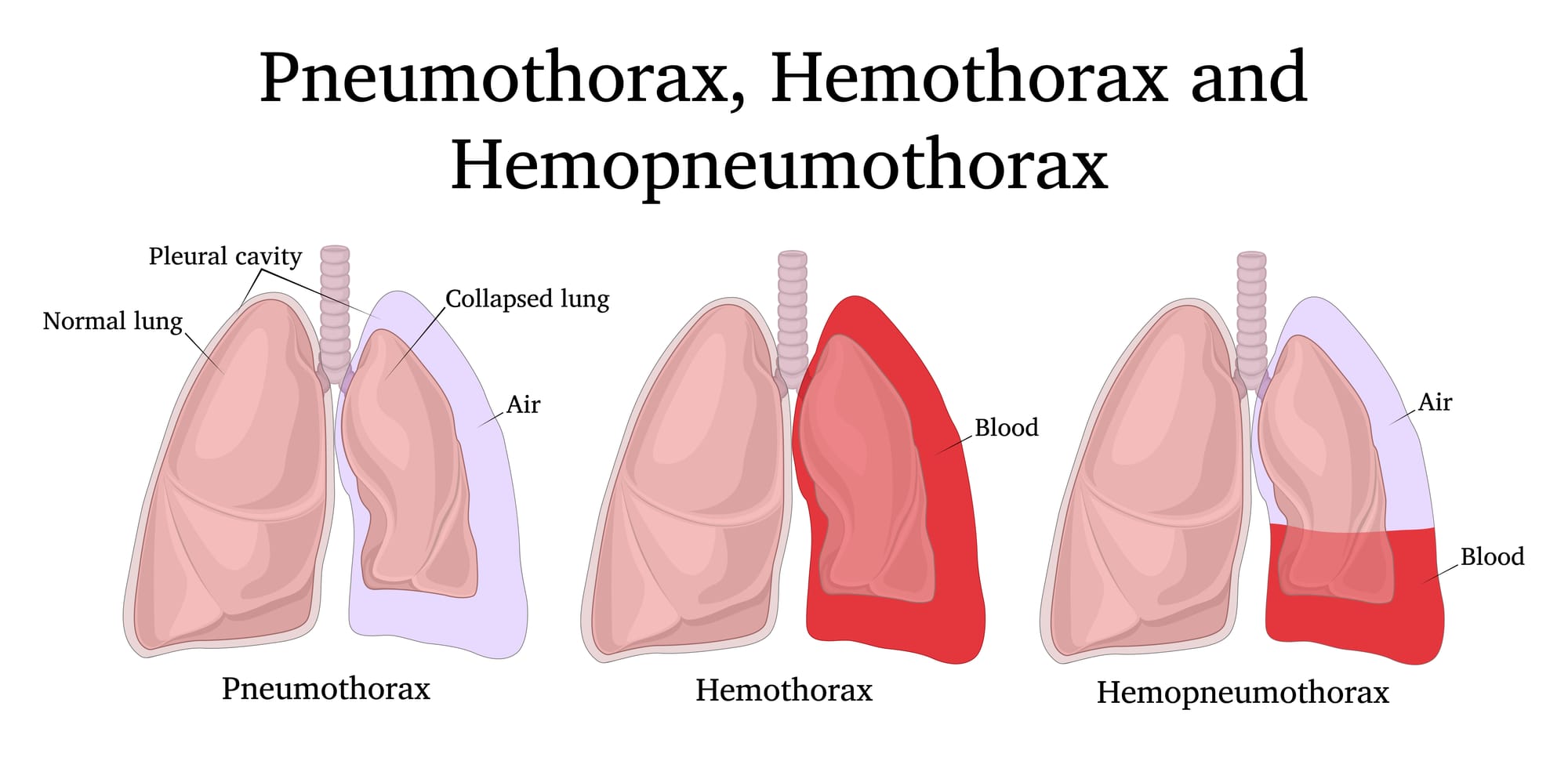
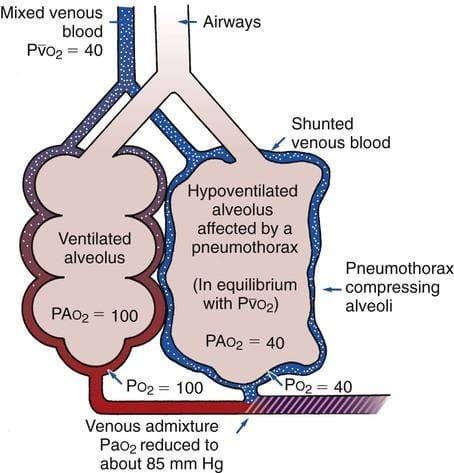
Pneumothorax is the collection of air outside the lungs within the pleural cavity, which is between the parietal and visceral pleura. Accumulation of air can put pressure on the lungs and lead to partial or complete collapse.
What are the types of pneumothorax and their causes?
There are 2 main types of pneumothorax [1]:
- Spontaneous pneumothorax is a collapsed lung that happens without an injury. It's further divided into:
- Primary spontaneous pneumothorax: No underlying health condition or disease causes the collapsed lung. This can happen if abnormal air pockets in your lungs (blebs) break apart and release air. Risk factors for primary spontaneous pneumothorax include:
- Smoking
- Tall, thin body habitus in an otherwise healthy person
- Pregnancy
- Marfan`s syndrome
- Family history of pneumothorax
- Secondary spontaneous pneumothorax: It happens in some lung conditions that cause blockages and trapped air, leading to bulging areas (bullae) that can burst. Lung conditions associated with secondary pneumothorax include:
- Chronic obstructive pulmonary disease (COPD)
- Asthma
- HIV with pneumocystis pneumonia
- Necrotizing pneumonia
- Tuberculosis
- Sarcoidosis
- Cystic fibrosis
- Bronchogenic carcinoma
- Idiopathic pulmonary fibrosis
- Langerhans cell histiocytosis
- Collagen vascular disease
- Inhalational drug use, like cocaine or marijuana
- Thoracic endometriosis
Severe ARDS
- Traumatic pneumothorax can be a result of injuries, accidents, or medical procedures. It is further classified into:
- Injury-related pneumothorax: can occur in case of rib fracture, knife, or gunshot injury in the chest area that may puncture the lung.
- Iatrogenic pneumothorax: Occurs when your lung is punctured during a medical procedure like a lung biopsy, tracheostomy, intercostal nerve block, or a central venous line insertion.
- Other rare types of pneumothorax include:
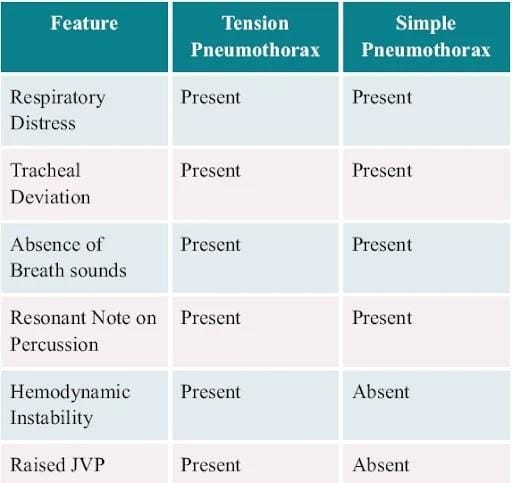
- Tension pneumothorax, where the air gets into the lungs but can`t get out. The one-way valve effect causes pressure to build up inside your chest. This is a serious form of pneumothorax that’s a medical emergency. Causes of tension pneumothorax may include:
- Penetrating or blunt trauma
- Barotrauma due to positive-pressure ventilation
- Percutaneous tracheostomy
- Conversion of spontaneous pneumothorax to tension
- An open pneumothorax when an occlusive dressing works as a one-way valve [2]
- Catamenial pneumothorax: A rare condition that can affect people with endometriosis. Endometrial tissue growing outside of your uterus can form cysts that can bleed into the pleural space, causing your lung to collapse.
How common is pneumothorax?
What are the symptoms of pneumothorax?
- Sharp chest or shoulder pain, made worse by a deep breath or a cough.
- Shortness of breath
- A dry, hacking cough
- Nasal flaring
- Bluish colour of the skin due to lack of oxygen (cyanosis)
- Chest tightness
- Easy fatigue
- Abnormal breathing patterns or increased effort of breathing
- Rapid heart rate
- Shock and collapse [3]
Light-headedness and near fainting
How is pneumothorax diagnosed?
Chest radiography, ultrasonography, or CT can be used for diagnosis, although diagnosis from a chest x-ray is more common. Radiographic findings of a 2.5 cm air space are equivalent to a 30% pneumothorax.
If a patient is hemodynamically unstable with suspected tension pneumothorax, intervention is not withheld to await imaging. Needle decompression can be performed based on a convincing history and physical exam, indicating a tension pneumothorax. [2]
What is the treatment for pneumothorax?

Treatment goals include:
- Relieving pressure on the lungs, allowing them to re-expand and
- To prevent recurrent lung collapse
For a small portion of lung collapse, the doctor may choose to monitor symptoms and do a series of X-rays until the lung has re-expanded. For severe pneumothorax cases:
- Needle aspiration: Excess air is syringed out through a needle catheter from the pleural space.
- Chest tube insertion: Air is removed continuously from the pleural space by a flexible chest tube attached to a device with a one-way valve.
Other non-surgical options are:
- Using an irritant around the lung tissue so that they'll stick together and seal any leaks. This can be done through the chest tube, or may be done during surgery.
- Drawing blood from your arm and placing it into the chest tube. The blood creates a fibrinous patch on the lung (autologous blood patch), sealing the air leak.
- Doing a bronchoscopy to look at your lungs and air passages, and placing a one-way valve. The valve allows the lung to re-expand and the air leak to heal.
Surgery can be done if other options fail to close the air leak. In most cases, through minor incisions, the surgeon can close air leaks using a tiny fibre-optic camera and narrow, long-handled surgical tools.
Rarely, the surgeon will have to make a larger incision between the ribs to get better access to multiple or larger air leaks. [4]