TREATMENT FOR MULTIPLE SCLEROSIS
TREATMENT FOR MULTIPLE SCLEROSIS
There is no cure for multiple sclerosis. Treatment typically focuses on speeding recovery from attacks, reducing new radiographic and clinical relapses, slowing the progression of the disease, and managing MS symptoms. Some people have such mild symptoms that no treatment is necessary.
What is the medical management of MS?
Glatiramer acetate, dimethyl fumarate, fingolimod, interferon-beta preparations, natalizumab, and mitoxantrone are some of the primary disease-modifying therapies. Immediate treatment initiation upon diagnosis is crucial for multiple sclerosis. Short-term goals focus on decreasing MRI lesion activity, while long-term goals aim to prevent secondary progressive multiple sclerosis. Post-treatment challenges include ensuring patient compliance and monitoring for drug toxicity.
In the realm of treatment and management for multiple sclerosis, several disease-modifying therapies, as mentioned below, offer various mechanisms to address the underlying pathology.
Glatiramer acetate: This is a synthetic polypeptide mixture that may act as a ligand for major histocompatibility complex molecules, limiting their activation and promoting regulatory cell induction. This drug may also have neuroprotective and repair mechanisms. Glatiramer acetate is administered subcutaneously and is generally well-tolerated; however, this drug is ineffective for progressive forms of multiple sclerosis.
Interferon-beta preparations: These preparations act through multiple mechanisms, including modulation of T- and B-cell function, cytokine expression alteration, potential role in blood-brain barrier recovery, and reduction in matrix metalloproteinase expression. The administration is subcutaneously or intramuscularly, and they may cause flu-like symptoms and possibly briefly worsen patients' neurological symptoms.
Natalizumab: This drug is an intravenously (IV) administered humanized monoclonal antibody that blocks leukocyte adhesion to vascular endothelial cells, thereby inhibiting leukocyte migration into the CNS. Although generally well tolerated, natalizumab may cause mild headaches, and flushing may occur during IV administration.
Mitoxantrone: This is an IV-administered chemotherapeutic agent used to treat multiple sclerosis due to its effects on DNA repair and RNA synthesis. A possible effect on cellular and humoral immunity may represent the therapy mechanism for multiple sclerosis. However, its use is limited due to the various adverse effects that have been documented, including amenorrhea and alopecia.

Fingolimod: This is an orally administered drug with immunomodulatory effects, possibly relating to the inhibition of T-cell migration. However, possible adverse effects include lymphopenia, bradycardia, and hepatotoxicity, thereby necessitating careful monitoring.
Patients with secondary progressive, progressive-relapsing, and primary progressive multiple sclerosis primarily experience neurodegenerative processes. Due to this, disease-modifying therapies show varying effectiveness, ranging from possible benefits to limited impact on disease progression. Typically, younger patients with a shorter duration of progression tend to benefit more from these therapies. (https://www.ncbi.nlm.nih.gov/books/NBK499849/)
What is the treatment for acute attacks of MS?
- Corticosteroids, such as oral prednisone and intravenous methylprednisolone, are prescribed to reduce nerve inflammation. Side effects may include insomnia, increased blood pressure, increased blood glucose levels, mood swings and fluid retention.
- Plasma exchange (plasmapheresis). The liquid portion of part of your blood (plasma) is removed and separated from your blood cells. The blood cells are then mixed with a protein solution (albumin) and put back into your body. Plasma exchange may be used if your symptoms are new, severe and haven't responded to steroids. (https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/diagnosis-treatment/drc-20350274)
Multiple sclerosis is a complex neurological disorder that leads to various neurological and non-neurological symptoms, disabilities, and complaints. A comprehensive team approach involves specialists from:
- Neurology and neuro-ophthalmology
- Psychiatry and cognitive psychology
- Pain management
- Nursing and physician assistants
- Speech therapy
- Occupational therapy
- Social work
- Physical medicine and rehabilitation
- Urology (in the setting of genitourinary complications)
- Gastroenterology (in the setting of gastrointestinal complications)
ROLE OF PHYSICAL THERAPY IN MS MANAGEMENT
(source: Physical rehabilitation by Susan O`sullivan, sixth edition)
- Sensory deficits and skin care: treatment is focused to enhance sensory awareness by training to compensate for sensory loss and promote safety. It is important to remember
that sensory deficits may remit, so ongoing examination is necessary. The success of compensatory training strategies depends on the availability of other intact sensory systems. Patients with proprioceptive losses demonstrate impairments in movement control and motor learning. They require increased use of other sensory systems, especially
vision. Tapping, verbal cueing, and/or biofeedback can all be effective forms of augmented feedback. Proprioceptive loading through exercise, light tracking resistance, resistance bands or weights, and the use of a pool may heighten residual proprioceptive function and improve
movement awareness.
Visual loss will interfere with movement and postural control. Blurred vision, especially at night or in low light situations, can occur after episodes of optic neuritis. When individuals with MS have to stand in an upright position in the dark, the likelihood of falls increases. It is therefore important to instruct the patient to maintain adequate lighting at all times
(e.g., use of a bright light at night) and reducing clutter to improve safety. Adding colour contrast between items in the environment (e.g., stair markings) can also improve safety. Double vision is frequently the result of impaired coordination and weak eye muscles.
It can be controlled by placing a patch over one eye and is an important strategy for improving reading, driving, or watching television.
Approximately 20% of patients with MS will develop a pressure ulcer during the course of the disease. Awareness, protection, and care of desensitized parts should be taught early in the rehabilitation process and consistently reinforced by all members of the team.
- Pain management: Pain can be classified into four categories: pain directly from MS, pain secondary to other symptoms of MS, pain as a result of drug treatment for MS, and pain independent of MS. The management of pain depends on an accurate determination of its causes. Patients may experience relief of pain with regular stretching or exercise, massage, and ultrasound. Postural retraining and correction of faulty movement patterns along with orthotic and/or adaptive seating devices can reduce malalignment and pain. Stabbing pain from Lhermitte’s sign may be relieved with a soft cervical collar to limit neck flexion. Stress management techniques, relaxation training, biofeedback, and meditation are often helpful in reducing both anxiety and pain.
- Aerobic conditioning: Determining an appropriate exercise prescription to improve cardiovascular conditioning needs to be carefully individualized for each patient. Recent studies have shown that peak VO2 and exercise capacity can be predicted through submaximal testing. Most individuals with MS can achieve 70-85% of their age-predicted HRmax. Recommended training frequency is 3 to 5 days/week, on alternate days. Daily exercise at lower levels of intensity is recommended for individuals with more limited exercise capacities (e.g., 3 to 5 metabolic equivalent [METs]).
Muscle strength and conditioning: exercises can be scheduled on alternate days and when body temperature is cooler to prevent fatigue with alternating use of upper and lower extremities and adequate rest periods between exercises. Precautions should be taken with certain impairments. Tactile and proprioceptive losses or incoordination and tremors may make the use of some equipment (e.g., free weights) unsafe. Visual feedback, when intact, should be used to monitor exercise performance. An alternative suggestion would be to use synchronized arm/leg ergometers to control limb movements.
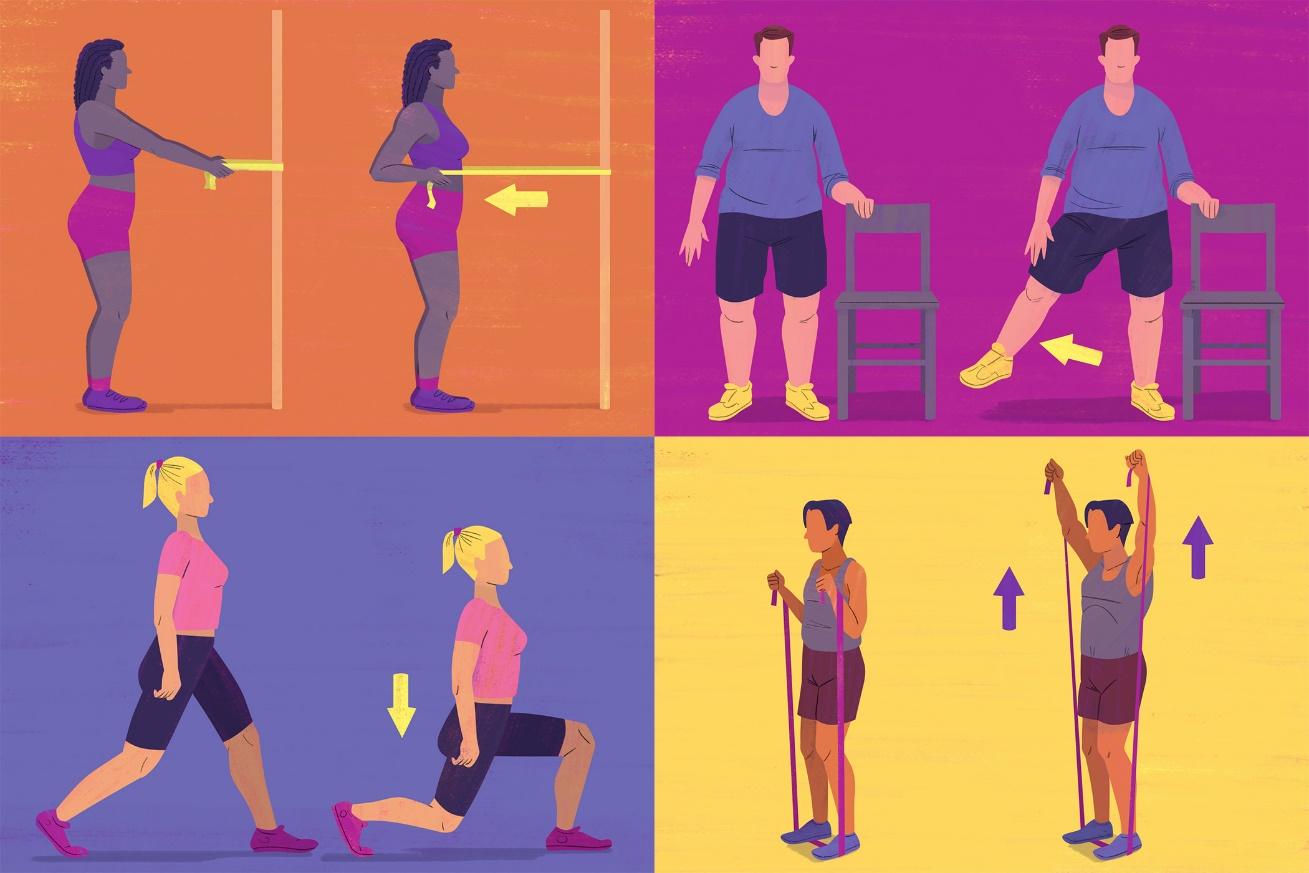
• Training intensity should be limited to 60% to 85% HRpeak or 50% to 70% peak VO2.
• Recommended duration is 30 minutes per session or, for more involved individuals, three 10-minute sessions per day.
• Type of exercise can include cycling, walking, swimming, or water aerobics.

- Managing fatigue: fatigue is often associated with thermal stress, which can be offset with adequate rest and the use of cooling and precooling treatments during exercise. Energy conservation refers to the adoption of strategies that reduce overall energy requirements of the task and overall level of fatigue. Activity pacing refers to the balancing of activity with rest periods interspersed throughout the day.
- Managing spasticity: AFOs are prescribed for foot drop, poor knee control (especially hyperextension), minimal to moderate spasticity, and poor somatosensation. Medication such as baclofen or ice packs may temporarily reduce spasticity. Functional activities aimed at reducing tone should concentrate on trunk and proximal segments, because many patterns of hypertonus seem to be fixed from the action of the stronger proximal muscles.
Balance and co-ordination: Cerebellar deficits leading to ataxia and postural instability are common in MS. Specific exercise techniques that can be used to promote stability include joint approximation applied through proximal joints (shoulders or hips) or spine, and rhythmic stabilization (PNF). Biofeedback training using augmented feedback can be used to improve balance function. Control of ataxic limb movements (tremor and dysmetria) can be achieved through proprioceptive loading and light resistance. Weighted canes or walkers can be used to reduce ataxic UE movements that interfere with the use of an assistive device during ambulation. Weighted spoons or forks can be used to enhance eating.

As an educator, the therapist has an important role in assisting the patient and family/caregivers in providing information on the following:
- The disease process, clinical manifestations, and their significance in terms of management.
- Prevention of secondary complications, indirect impairments, and activity limitations.
- The rehabilitation process, the POC, and its specific interventions.
- The HEP, including interventions that can be carried out independently.
- Monitoring the effects and possible adverse reactions of medications.
- Use of assistive devices and adaptive equipment.
- General health and stress management techniques.
- Prompt referral to community resources including a support group can provide a necessary stabilizing base for patients and their families/caregivers.