PEPTIC ULCER
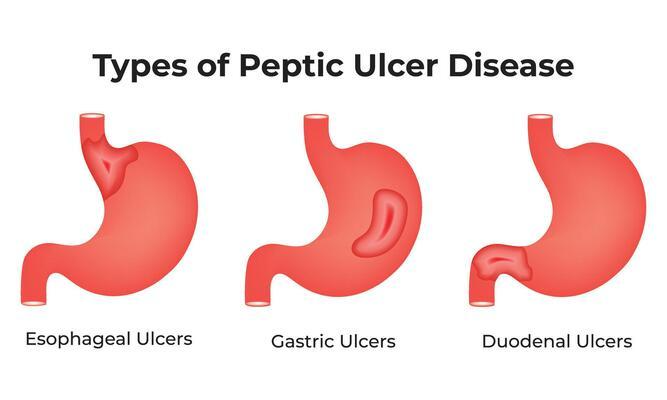
Peptic ulcer (PU) disease is characterized by discontinuation in the inner lining of the gastrointestinal (GI) tract because of gastric acid secretion or pepsin. It extends into the muscularis propria layer of the gastric epithelium. It usually occurs in the stomach and proximal duodenum. It may also be located in the lower esophagus, distal duodenum, or jejunum which determines the type of ulcer.
How common is PU disease?
Between 5% and 10% of people worldwide will develop peptic ulcer disease (PUD) in their lifetimes. It can develop at any age, though it’s more common in middle-aged adults. It’s also more common in males.
What are the symptoms of PU?
Most common symptoms people report are epigastric pain (central upper abdominal pain) and indigestion or dyspepsia. Indigestion describes a combination of symptoms that occur after eating and during digestion. It includes epigastric pain with a notable burning quality, combined with a feeling of fullness that comes on shortly after eating and/or lasts a long time after.
A burning sensation is the feeling of stomach acids and enzymes eating through your gastrointestinal lining which can be localized. A stomach ulcer will often feel worse shortly after a meal (within 30 minutes), when gastric juices are at their peak. A duodenal ulcer may feel better shortly after a meal. But you’ll feel it more about two to three hours later, when the food and digestive juices enter your duodenum.
Many people with duodenal ulcers report pain that awakens them at night. This can also occur with jejunal ulcers. Jejunal pain will be a little lower, closer to your belly button. If you have an esophageal ulcer, it might feel like heartburn which peaks at night. Other symptoms include:
- Bloated stomach
- Burping or belching
- Loss of appetite
- Nausea and vomiting
Some people don’t show symptoms until the disease causes extra complications such as:
- Blood in stools
- Black, tarry stool
- Coffee ground vomitus
- Dizziness or faintness
- Pallor (paleness)
- Rapid heart rate
Untreated ulcers may begin to bleed or may continue to wear through your GI tract until there’s a hole causing:
- Sudden, sharp and severe abdominal pain
- Abdominal swelling and tenderness to touch
- Fever and chills
Some people develop so much scarring and/or swelling from untreated ulcers in their GI tract that it can slow or stop food from moving through causing:
- Abdominal bloating, swelling and pain.
- Nausea and vomiting.
- Loss of appetite and weight loss.
- Loss of bowel movements and constipation. (https://my.clevelandclinic.org/health/diseases/10350-peptic-ulcer-disease)
What are the causes of peptic ulcer?
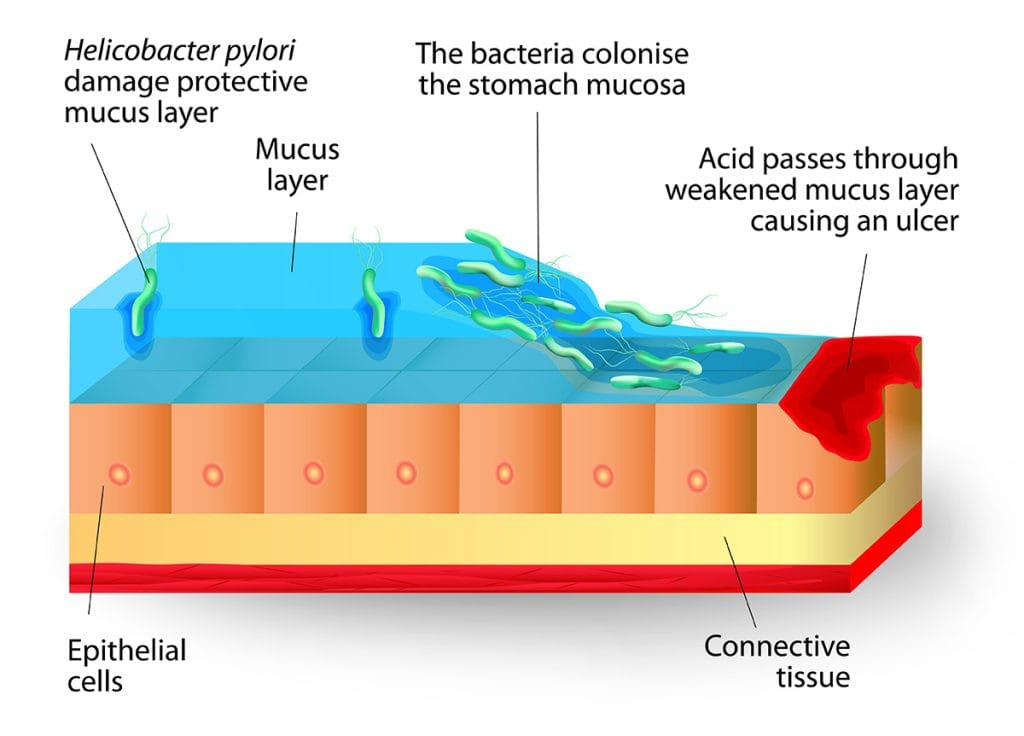
Your digestive tract is coated with a mucous layer that most often protects against acid. But if the amount of acid increases or the amount of mucus decreases, you could develop an ulcer. The 2 most common reasons to get PU are:
- Helicobacter-Pylori infection: H. pylorus is a gram-negative bacillus that is found within the gastric epithelial cells. This bacterium is responsible for 90% of duodenal ulcers and 70% to 90% of gastric ulcers. H. pylori infection is more prevalent among those with lower socioeconomic status and is commonly acquired during childhood. The organism has a wide spectrum of virulence factors, allowing it to adhere to and inflame the gastric mucosa. This results in hypochlorhydria or achlorhydria, leading to gastric ulceration.
- NSAID use: Nonsteroidal anti-inflammatory drug use is the second most common cause of PUD after H. pylori infection. The secretion of prostaglandin normally protects the gastric mucosa. NSAIDs block prostaglandin synthesis by inhibiting the COX-1 enzyme, resulting in decreased gastric mucus and bicarbonate production and a decrease in mucosal blood flow.
- A part from NSAIDs, corticosteroids, bisphosphonates, potassium chloride, and fluorouracil have been implicated in the etiology of PU.
- Less common causes of PU may include:
- Zollinger-Ellison syndrome
- Malignancy (gastric/lung cancer, lymphomas)
- Stress (Acute illness, burns, head injury)
- Viral infection
- Vascular insufficiency
- Radiation therapy
- Chemotherapy
- Crohn`s disease (https://www.ncbi.nlm.nih.gov/books/NBK534792/)
How is PU diagnosed?
Medical history and physical examination may require additional tests to support the diagnosis of PU.
- A blood, stool or breath test can show whether H. pylori is in your body.
- Endoscopy involves passing the endoscope, down your throat and into your esophagus, stomach and small intestine to look for ulcers.
If there's an ulcer, your health professional may remove a small tissue sample for study in a lab. This is called a biopsy. A biopsy also can show whether H. pylori is in your stomach lining.
- Series of X-rays of the esophagus, stomach and small intestine are taken after swallowing liquid barium. The liquid coats your digestive tract and makes an ulcer easier to see.
How is PU treated?
Treatment for peptic ulcers involves killing the H. pylori germ, if needed. Treatment also might involve stopping NSAIDs or lowering the amount, if possible, and taking medicine to help the ulcer heal.
- Medicines to kill H. Pylori may include amoxicillin (Amoxil, Larotid), clarithromycin (Biaxin XL), metronidazole (Flagyl, Likmez), tinidazole (Tindamax), tetracycline and levofloxacin.
- Proton pump inhibitors (PPIs) reduce stomach acid. PPIs include omeprazole (Prilosec), lansoprazole (Prevacid), rabeprazole (Aciphex), esomeprazole (Nexium) and pantoprazole (Protonix).
Long-term or high-dose use of proton pump inhibitors may increase your risk of hip, wrist and spine fracture. Ask your healthcare professional whether a calcium supplement may reduce this risk.
- Medicines to reduce stomach acid called histamine (H-2) blockers, help relieve ulcer pain and help with healing. Acid blockers include famotidine (Pepcid AC), cimetidine (Tagamet HB) and nizatidine (Axid AR).
- Cytoprotective agents like sucralfate (Carafate) and misoprostol (Cytotec) are known to protect the lining of the stomach and small intestine.
If the ulcer is not healing (refractory ulcers), an endoscopy may be required during follow-up. Reasons for refractory ulcers include:
- Not taking medicines as prescribed.
- Having a type of H. pylori that resists antibiotics.
- Often using pain relievers, such as NSAIDs, that increase the risk of ulcers.
Treating refractory ulcers involve getting rid of the cause for e.g. using a more suitable anti-biotic for resistant bacteria or smoking cessation as smoking causes delayed ulcer healing. A serious complication from an ulcer, such as bleeding or a hole in the stomach, may need treatment with endoscopy or surgery. But because there are many medicines that work well, people with peptic ulcers need surgery far less often than in the past. (https://www.mayoclinic.org/diseases-conditions/peptic-ulcer/diagnosis-treatment/drc-20354229)