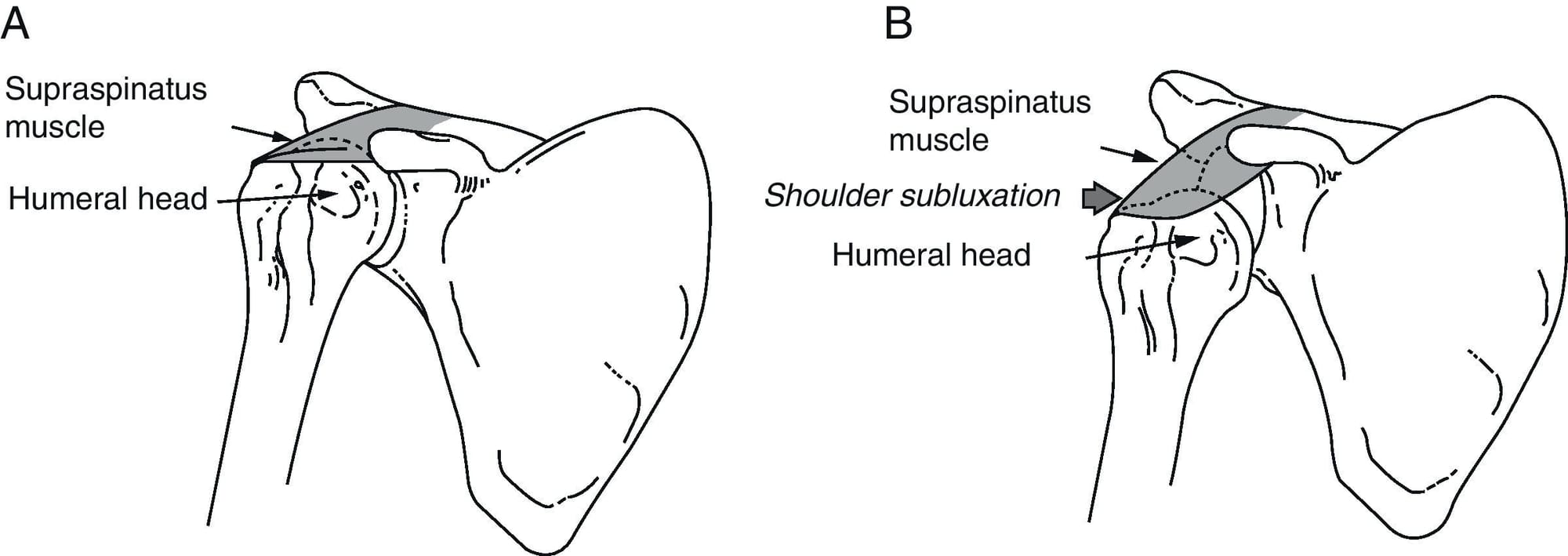
Shoulder Subluxation
Shoulder subluxation is defined as partial or incomplete dislocation of the glenohumeral joint or translation between the humeral head and glenoid fossa while the humeral head is in contact with the glenoid fossa. The weakness of rotator cuff muscles or laxity of the glenohumeral ligaments causes the humeral head to slip out of the glenoid fossa easily and results in glenohumeral subluxation.
What is the etiology of shoulder subluxation?
The etiology can be classified as traumatic, non-traumatic, and neuromuscular causes.
- For the traumatic cause, it is more frequent in active young individuals. Shoulder subluxation is prevalent in boxers. However, a non-contact sport with repetitive shoulder movements and a hand in the outstretched position can also cause subluxation.
- For the non-traumatic cause, the etiology could be multifactorial. The patients may have suboptimal shoulder muscle control or tendon/ligament injury in the rotator cuff interval.
These 2 patterns of shoulder instability can be defined as TUBS syndrome (traumatic, unilateral dislocations with a Bankart lesion, often requiring surgery) and AMBRI syndrome (atraumatic, multidirectional, bilateral shoulder subluxation/dislocations, often treated with rehabilitation, and sometimes requiring inferior capsular shift), respectively.

- The neuromuscular causes, such as stroke, cerebral palsy, and brachial plexus injury, can also lead to shoulder subluxation. (https://www.ncbi.nlm.nih.gov/books/NBK507847/)
What are the symptoms of shoulder subluxation?
The presenting symptoms maybe stiffness, mild pain, and instability of the shoulder girdle. A history of previous dislocation, mechanism of injury (direction of shoulder movements during the traumatic event), and family history of shoulder instability are also important.
For stroke patients with hemiplegia, although there is no clear association between shoulder subluxation and pain, both medical conditions can exist simultaneously. If they present with concomitant subluxation and shoulder pain, the physical examination for the rotator cuff tendinopathy, acromioclavicular arthropathy, and subacromial impingement helps identify the cause of shoulder pain. Furthermore, some patients have a limited range of motions on the hemiplegic shoulder after shoulder subluxation. (https://www.ncbi.nlm.nih.gov/books/NBK507847/)
What are the grades of shoulder displacement?

Hawkins et al recommended a classification based on millimetres. Grade 0 is defined as no translation; grade I represents a translation smaller than 1 cm; grade II is considered when there is a moderate translation of 1 to 2 cm (or up to the glenoid rim) and grade III equals severe translation of more than 2cm or over the glenoid rim.
A more popular method widely used in clinical practice also described by Hawkins and includes four grades; Grade 0: no translation, grade I: translation to the glenoid rim, grade II: translation of the head over the glenoid rim and grade III, when the head stays out of the joint after removing the examiner hands. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5646139/)
What is included in physical examination of the shoulder for diagnosing subluxation?
During physical examination, subluxation is detected by palpation of the glenohumeral joint. The extent of shoulder subluxation can be quantified by the distance from the acromion to the humeral head, using fingerbreadth, calliper, or tape. However, the physical examination should be performed bilaterally, and a comparison between both sides is important for establishing a correct diagnosis. Inspection of shoulder contours, the examination of the active and passive range of motion, and motor and sensory testing are suggested to determine the causes of shoulder subluxation.
The tests to examine shoulder laxity include the load and shift, drawer, sulcus, hyperabduction, and push-and-pull tests. The apprehension and relocation test are specific for examining anterior shoulder instability. (https://www.ncbi.nlm.nih.gov/books/NBK507847/)
How is shoulder subluxation treated?
Non-surgical treatment: In traumatic shoulder subluxation, the immediate treatments include ice packing to reduce soft tissue swelling, avoiding postures leading to recurrent subluxation, and wearing a protective arm sling. Narcotics or non-steroid anti-inflammatory drugs can be used for pain control. The passive or active assistive range of motion exercise of the upper limb and scapular stabilization exercise can start as early as possible, followed by strengthening of shoulder girdle muscles and glenohumeral joint proprioceptive training to improve dynamic shoulder stability.

Shoulder exercises need to be considered into 2 categories; closed kinetic chain and open kinetic chain. Exercises which involve weight being placed through the arm with the hand fixed on a surface, closed chain exercises, facilitate co-contraction of the rotator cuff (RC) and deltoid muscles, thereby enhancing joint stability, stimulating muscular co-activation and proprioception.
Initially RC exercises should be performed with a stable body posture and the weight of the arm supported on a table, floor or wall to encourage muscular co-activation and scapula stability without increasing shear forces across the shoulder joint. Such positions may also provide guidance and reassurance to the patient as to where the shoulder feels more stable. In addition, closed chain exercises have been shown to encourage recruitment of the scapula thoracic muscles, so if specific weakness has been found in middle and lower trapezius and or serratus anterior such exercises can be beneficial.

In those patients who are unable to gain selective RC recruitment due to poor trunk stability and poor scapula position, exercises to improve postural tone may be beneficial. Destabilising the base of support and challenging their postural muscles such as sitting on a Swiss ball standing on one leg or on a wobble board may encourage postural muscles to engage and reduce inappropriate over-activity of muscles such as Latissimus Dorsi. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5611703/)

Specific rehabilitation of scapula muscles would be required if selective weakness is identified and this appears to be the primary driver to the glenohumeral instability. Scapula imbalance is widely recognised in shoulder pathology. Selective activation of the weaker muscle having minimal activity and inhibiting the hyperactive muscles is key in resolving symptoms. In athletes with anterior instability, the shoulder often shows dominance of upper trapezius against lower & middle trapezius and serratus anterior muscles. In patients with drooping scapula and poor upward rotation, increased activation of upper trapezius may be desirable.
If patients present with RC weakness in the outer range, or demonstrate scapula winging, lying supine is the preferred starting position to stabilise the trunk and scapula. Once the patient has achieved good activation and balance of the rotator cuff muscles, task specific functional exercises should be performed. Examples can include moving a ball clockwise/anti-clockwise on a wall, stabilising a ball on a wall, throwing and catching at speed, drop and catch, throwing at a target. Combining upper limb control with lower limb stability can start to incorporate patterns of muscle recruitment. Task specific activities have been shown to be effective in cognitive motor retraining.


If the patient is struggling to do basic exercises, then 3 further modalities can be used; elastic therapeutic tape, biofeedback and functional electrical stimulation. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5611703/)
Surgical treatment: Surgical management is considered in younger patients or active individuals with chronic shoulder subluxations. The indications for the operation include failed non-operative treatment, recurrent dislocation in younger age, irreducible dislocation, open dislocation, unstable reduction, the first time in young adults with traumatic unilateral dislocations, high work demand, and bony Bankart lesion.
The surgical procedures are classified into arthroscopic and open surgeries. Open shoulder stabilization surgery is needed if there is a contraindication for arthroscopic management like Hill-Sachs lesions, glenoid defects of more than 30%, humeral avulsion glenohumeral ligament (HAGL) injury, shoulder instability with the bony fragment, shoulder deformity and previous surgery of shoulder stabilization.
When comparing the results of open and arthroscopic surgeries, arthroscopic management is as effective as open repair in improving shoulder stability. The advantages of arthroscopic surgery include shorter operative time and hospital stay, decreased morbidities, and complications, lower cost, and less surgical scar. However, this arthroscopic technique highly depends on surgeons’ experiences and is not able to correct the bony defect. (https://www.ncbi.nlm.nih.gov/books/NBK507847/)