Pulmonary Hypertension: Symptoms, diagnosis, and treatment
PULMONARY HYPERTENSION
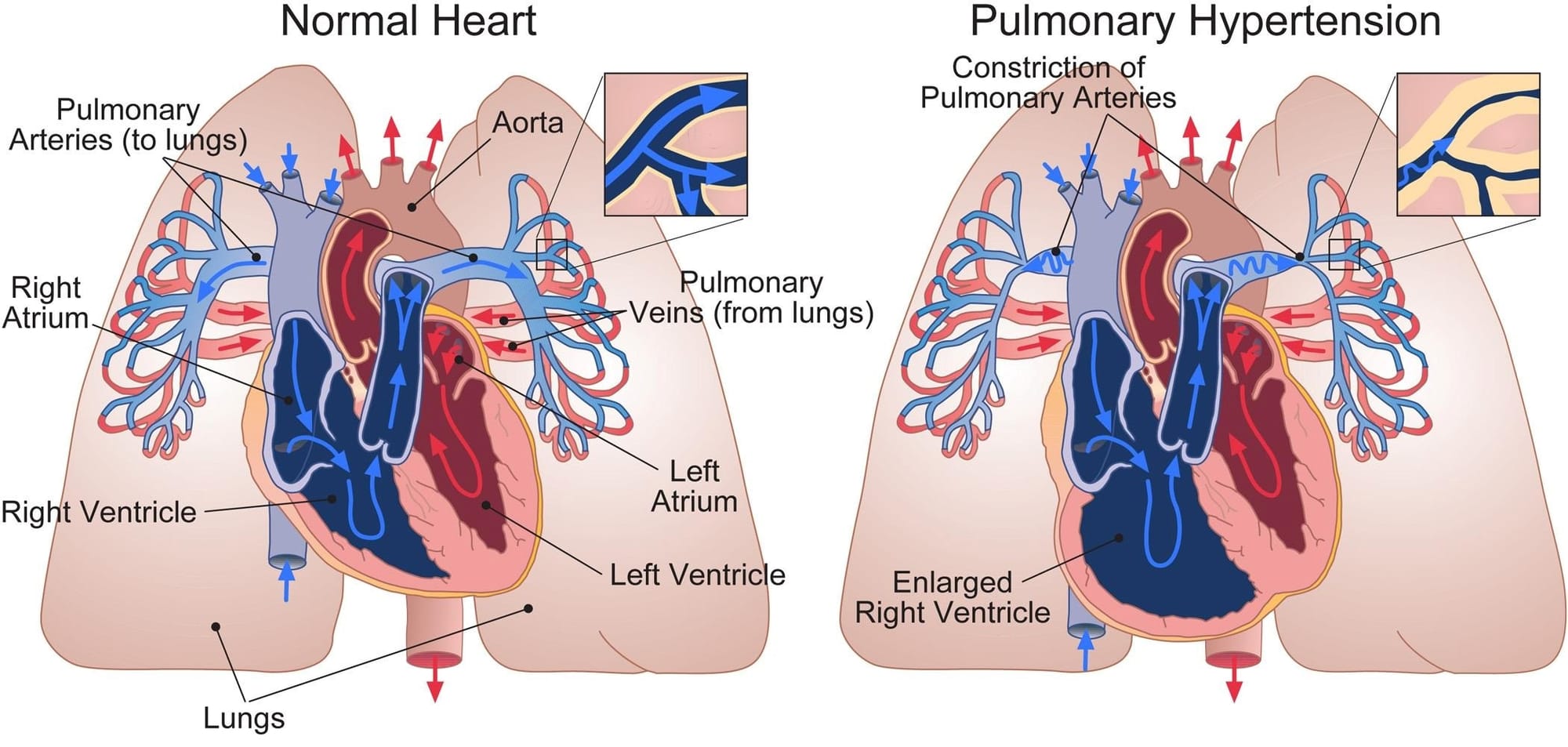
Pulmonary hypertension (PH) is a general diagnosis indicating high blood pressures in the lung arteries. These arteries carry oxygen-poor blood from your heart to your lungs. PH is dangerous because it disrupts the flow of blood through heart and lungs. High blood pressure in your pulmonary arteries causes these arteries to become narrow. As a result, your heart must work harder to pump oxygen-poor blood to your lungs. Over time, if left untreated, it can damage the heart.
What are the types of PH?
The World Health Organization classifies PH into 5 groups based on the cause:
How common is PH?
We don’t know exactly how many people around the world have pulmonary hypertension. But some estimates show PH may affect 1 in 100 people. This means 50 million to 70 million people are living with PH.
PH is even more common among older adults. Around the world, about 1 in 10 adults over age 65 have PH. PH affects:
- Nearly 100% of people with severe mitral valve disease
- About 65% of people with aortic valve disease
- Up to 30% of people with scleroderma
- About 20% to 40% of people with sickle cell disease
- About 1 in 200 people with HIV (https://my.clevelandclinic.org/health/diseases/6530-pulmonary-hypertension-ph)
What are the symptoms of PH?
The symptoms of pulmonary hypertension develop slowly. You may not notice them for months or even years. Symptoms get worse as the disease continues. Symptoms of PH include:
- Shortness of breath. It may first start during exercise and eventually happen at rest.
- Blue or grey skin. Depending on skin color, these changes may be harder or easier to see.
- Chest pressure or pain.
- Dizziness or fainting.
- Fast pulse or pounding heartbeat.
- Fatigue.
- Swelling in the ankles, legs and belly area. (https://www.mayoclinic.org/diseases-conditions/pulmonary-hypertension/symptoms-causes/syc-20350697)
How is PH diagnosed?
The evaluation process should include a comprehensive medical and family history, physical examination, monitoring of blood pressure, heart rate, oxygen saturation, and
- Laboratory tests: should include hematology studies, renal function tests, liver function tests (LFTs), iron profiles, and thyroid studies.
- Electrocardiogram: A normal ECG does not exclude the diagnosis of pulmonary hypertension. However, an abnormal ECG may indicate severe disease, especially if QRS and QTc are prolonged.
- Chest X-ray: Chest radiography may reveal underlying pulmonary hypertension, such as right atrial enlargement, pulmonary artery enlargement, peripheral vessel pruning, and a water bottle-shaped cardiac silhouette. Signs of left heart disease like Kerley B lines, pleural effusions, and left heart enlargement may also be present. Patients with lung disease may have diaphragmatic flattening, hyperlucency, volume loss, or reticular opacifications on x-ray, depending on their condition. A normal chest X-ray does not rule out pulmonary hypertension.
- Pulmonary function tests and arterial gases: Most patients with PAH have decreased carbon monoxide diffusion capacity (DLCO). A DLCO of less than 45% is associated with poor outcomes. Patients with PAH usually have a low normal or slightly low partial pressure of oxygen (PaO2).
- Chest CT and digital subtraction angiography: helps to identify interstitial lung diseases and measure enlarged arteries or heart chambers.
- Echocardiographic assessment should only be used to estimate pulmonary hypertension probability. RHC is used for diagnostic confirmation and therapeutic guidance.
- Cardiopulmonary exercise testing: In patients with PAH, a low end-tidal partial pressure of carbon dioxide, high ventilatory equivalent for carbon dioxide, low oxygen pulse, and low peak oxygen uptake are typically seen.
- Cardiac MRI: is an incredibly powerful tool that accurately assesses atrial and ventricular function and morphology. This modality can also measure blood flow through the vena cava, pulmonary artery, and aorta, allowing for stroke volume quantification. The test is sensitive for detecting early pulmonary hypertension but does not reliably estimate pulmonary artery pressures.
- Abdominal ultrasonography: The main reason for obtaining an abdominal ultrasound is to detect liver abnormalities, portal hypertension, and kidney injury that may arise from chronic pulmonary hypertension. Ultrasonography can help assess the extent of the collateral damage to these organs.
- Right heart catheterization: not only confirms the diagnosis of PH but also yields enormous information, including right- and left-sided filling pressures, pulmonary artery pressure, PAWP, PVR, and cardiac output.
- Genetic testing/ counselling, sleep study and lung biopsy are a few other tests that may help to confirm diagnosis. (https://www.ncbi.nlm.nih.gov/books/NBK482463/)
Ventilation-perfusion scanning: to rule out CTEPH (chronic thromboembolic pulmonary hypertension) in patients with pulmonary hypertension.
How is PH treated?
Medication
- Vasodilators like epoprostenol (Flolan, Veletri), treprostinil (Remodulin, Tyvaso, others), iloprost and selexipag (Uptravi) can be either injected intravenously or given orally.
- Soluble guanylate cyclase stimulators like riociguat (Adempas) relaxes the pulmonary arteries and lowers pressure in the lungs.
- Endothelin receptor antagonists such as bosentan (Tracleer), macitentan (Opsumit) and ambrisentan (Letairis) reverse the effect of a substance in the walls of blood vessels that causes them to narrow.
- Phosphodiesterase 5 (PDE5) inhibitors such as sildenafil (Revatio, Viagra) and tadalafil (Adcirca, Alyq, Cialis) may be used to increase blood flow through the lungs. These medicines also are used to treat erectile dysfunction.
- High dose calcium channel blockers such as amlodipine (Norvasc), diltiazem (Cardizem, Tiazac, others) and nifedipine (Procardia) help relax the muscles in the walls of blood vessels.
- Anti-coagulants or blood thinners such as warfarin, help prevent blood clots.
- Digoxin helps the heart beat stronger and pump more blood. It can help control irregular heartbeats.
- Diuretics help the kidneys remove excess fluid from the body. This reduces the amount of work the heart has to do. Diuretics also may be used to reduce fluid buildup in the lungs, legs and belly area.
- Oxygen therapy may be suggested if you live at a high altitude or have sleep apnea. Some people with pulmonary hypertension need oxygen therapy all the time.
Surgery
If medicines do not help control the symptoms of pulmonary hypertension, surgery may be recommended.
- In an atrial septostomy, a doctor creates an opening between the upper left and right chambers of the heart. The opening reduces the pressure on the right side of the heart. Potential complications include irregular heartbeats called arrhythmias.
- Sometimes, a lung or heart-lung transplant may be needed, especially for younger people who have idiopathic pulmonary arterial hypertension. After a transplant, medicine must be taken for life to prevent the body from rejecting the new organ. (https://www.mayoclinic.org/diseases-conditions/pulmonary-hypertension/diagnosis-treatment/drc-20350702)