Pleural Effusion: Causes, Symptoms, Diagnosis, and Treatment
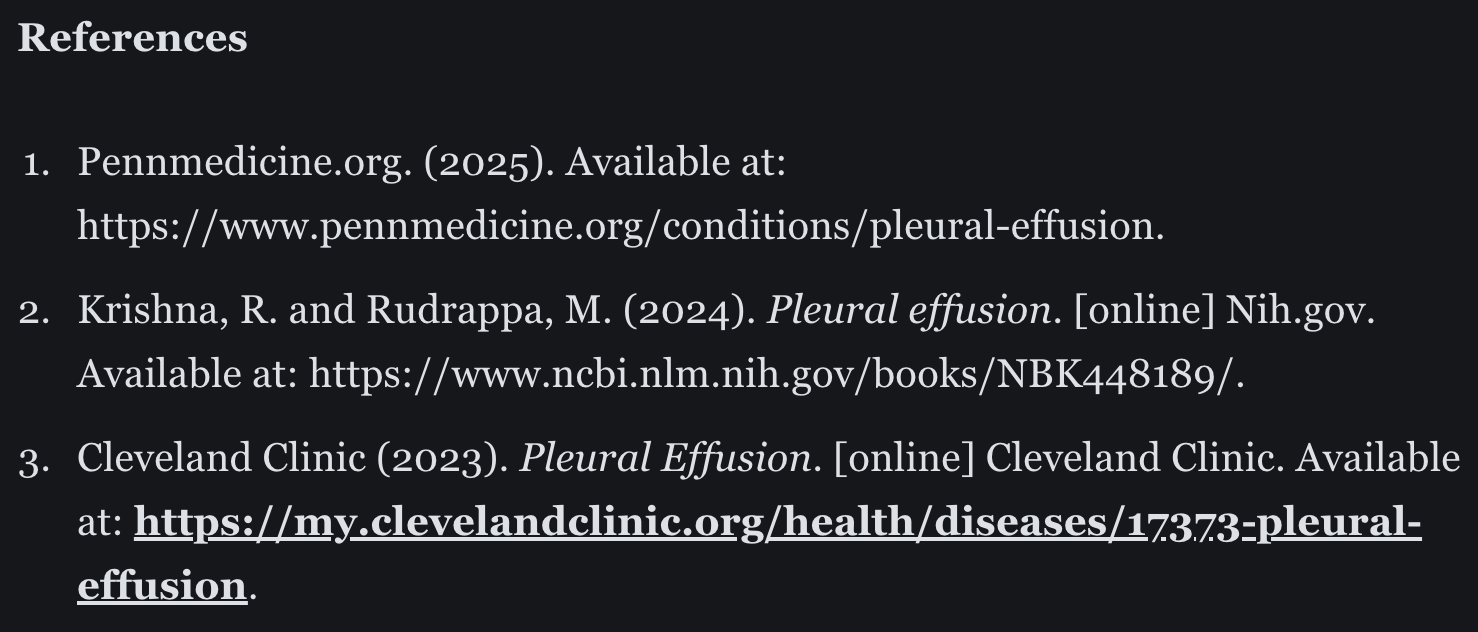
The body normally produces pleural fluid in small amounts to lubricate the surfaces of the pleura. This is the thin tissue that lines the chest cavity and surrounds the lungs. Pleural effusion (PE) is an abnormal, excessive collection of this fluid.
What are the types and causes of PE?
There are 2 types of PE:
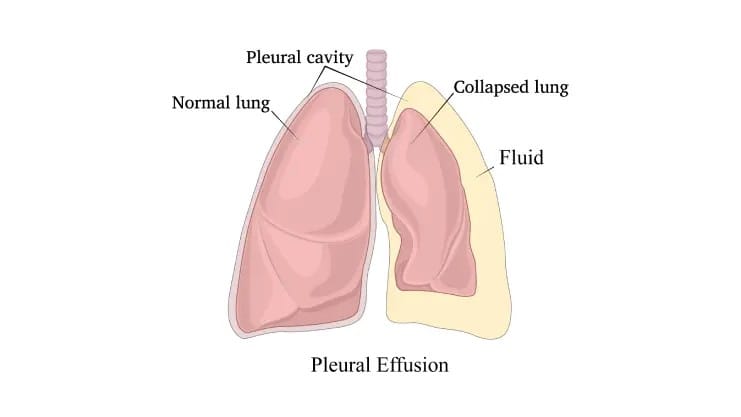
- Transudative PE is caused by fluid leaking into the pleural space due to increased pressure in the blood vessels or a low blood protein count. Heart failure is the most common cause. Other causes may be cirrhosis and nephrotic syndrome.
- Exudative effusion is caused by blocked blood vessels or lymph vessels, inflammation, infection, lung injury, recent open-heart surgery, or tumors. [1]
How common is pleural effusion?
According to the National Library of Medicine, more than 1.5 million people are diagnosed with pleural effusion in the United States each year. [2]
What are the less common causes of PE?
- Tuberculosis
- Autoimmune disease
- Bleeding from chest trauma
- Chylothorax (chyle from your lymphatic system after trauma)
- Rare chest or abdominal infections
- Exposure to asbestos
- Oesophageal rupture
- Pancreatitis
- Meig`s syndrome (from a benign ovarian tumor)
- Ovarian hyperstimulation syndrome
- Certain medications
- Abdominal surgery
- Radiotherapy
What are the symptoms of PE?
- Chest pain: Coughing or deep breathing makes it worse.
- Dyspnea: shortness of breath, or difficult, laboured breathing.
- Orthopnea: the inability to breathe easily unless you’re sitting up straight or standing up straight.
Some people with pleural effusion have no symptoms. They find out they have pleural effusion when they have a chest X-ray for another reason. [3]
How is PE diagnosed?
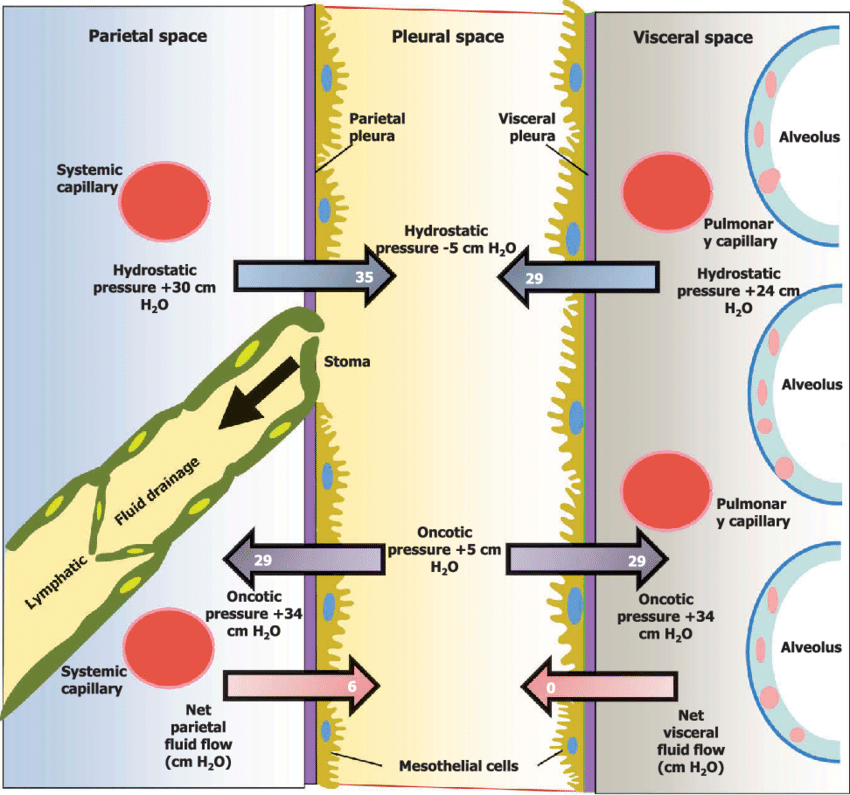
Chest X-ray: A meniscus sign on an upright posteroanterior chest X-ray is indicative of pleural fluid exceeding 200ml. Blunting of the costophrenic angle is also seen on the X-ray.
The lateral decubitus view can detect as little as 50 ml of fluid in the pleural space.
- Ultrasound is more sensitive in diagnosing and confirming effusion. Pleural fluid appears hyperechoic on ultrasound.
- Thoracentesis is almost always indicated in all PE cases to find the underlying cause unless heart failure is already diagnosed.
- A complex-appearing fluid collection seen in imaging necessitates planning for chest tube thoracostomy.
- Fluid extracted from thoracentesis should be tested for pH levels, serum protein levels, fluid and serum lactate dehydrogenase (LDH) levels, fluid glucose levels, fluid cell count differential, fluid gram stain, and culture. [2]
How is PE treated?
Medication to treat PE may include:
- Diuretics
- Heart failure medicines
- Antibiotics
- In case of malignancy, chemotherapy and/or radiotherapy
Other procedures:
- Thoracentesis: A chest tube is used to drain a pleural effusion that’s causing respiratory symptoms.
- Pleural sclerosis: For recurrent effusion, a sclerosing agent (a type of drug that purposely creates scarring) is put into your pleural cavity through a chest tube. This causes fibrosis (excessive fibrous tissue) of the pleura (pleural sclerosis). This is 50% successful in preventing pleural effusions from happening again.
Surgery:
- Video-assisted thoracoscopic surgery: With minimal incisions, VATS can manage pleural effusions that are difficult to drain or that come back because of a tumor.
- Thoracotomy: it is also known as an open thoracic surgery done in case of infections. A thoracotomy removes all of the fibrous tissue and helps clear out the infection from the pleural space. A chest tube is kept for a few days after surgery to drain the pleural fluid. [3]