Pancoast Tumor: Causes, Diagnosis, and Treatment
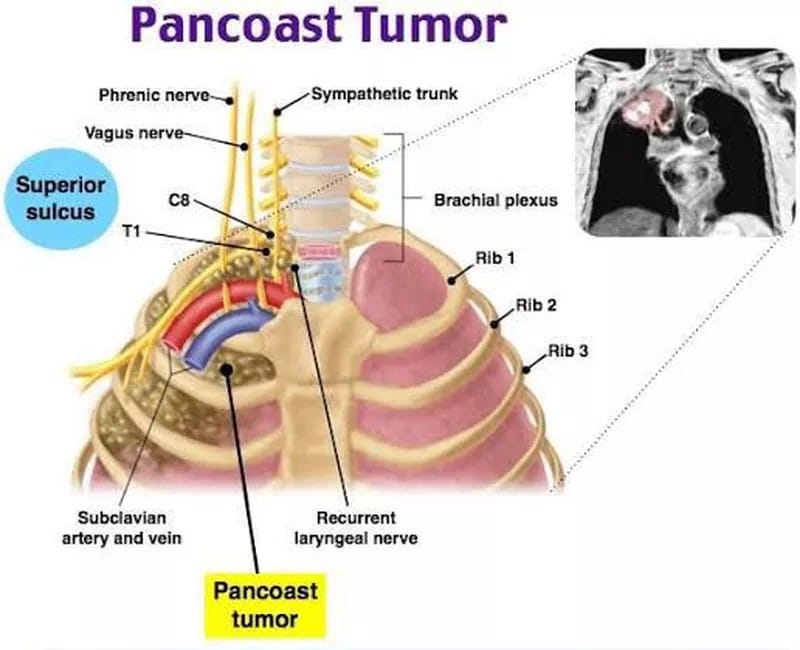
Pancoast tumors (PT) are defined as tumors that invade any of the structures at the apex of the chest, including the first rib or periosteum, the lower nerve roots of the brachial plexus, the sympathetic chain near the apex of the chest, or the subclavian vessels. Pancoast tumors occur in the apical portion of the lung, representing 3%–5% of all lung cancers.
Pancoast tumor is also known as a superior sulcus tumor. Histopathologically, these tumors are commonly adenocarcinomas, and less frequently, squamous call cancer. [1]
What causes PT?
Causes and risk factors of PT are similar to other lung cancer tumors. Common risk factors include smoking or exposure to second-hand smoke, long-term exposure to certain substances, including asbestos, radon gas, and heavy metals.
What are the symptoms of PT?
PT symptoms appear on the affected side of your body. Symptoms also depend on the structures involved in the upper thoracic region. [2]
- Severe shoulder pain, which may include pain in your shoulder blade.
- Pain that radiates down your arm and stops at your wrist, just above your little finger.
- Arm and hand weakness.
- Neck pain.
- Pain in the upper ribs.
- Upper arm swelling.
- Loss of dexterity in your hand and fingers.
- Tingling or numbness in the hand.
- Tiredness or fatigue.
- Tightness in your chest.
- Unexplained weight loss.
Up to 50% of people who have PT may also develop Horner`s syndrome, which may cause:
- Facial flushing
- A droopy eyelid (ptosis)
- Displaced eyeball (enophthalmos)
- Lack of sweat (anhidrosis) [2]
How is PT diagnosed?
Physical examination of the upper thoracic region and its contents is vital, which includes but is not limited to the following:
- Upper respiratory lobes/segments examination
- Musculoskeletal examination of the neck and both shoulders
- Assessment of lymph nodes
- Cranial nerve testing
Neurologic examination of both upper extremities
Pancoast tumor constitutes a group of malignancies (as it is classified based on location), hence a series of tests may help diagnose its status:
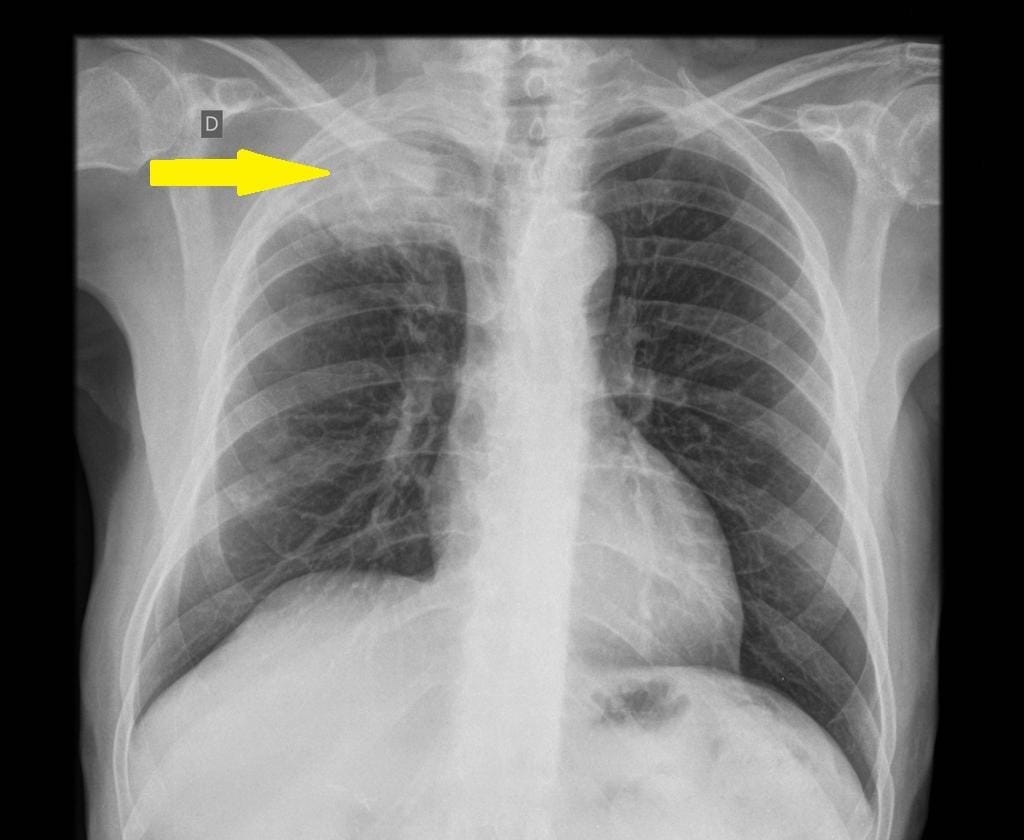
- An Initial plain chest x-ray is generally used to screen a patient with suspected or as an incidental finding showing soft tissue opacity at the apex of the lung (unilateral), or just an asymmetry in the apices greater than 5 mm can be noted. It may be difficult to appreciate findings in the early stages due to overlapping adjacent bony shadows.
- A CT scan provides more information on the extent of the primary tumor, mediastinal lymphadenopathy, and satellite tumors. A CT scan has poor sensitivity and specificity for accurate local staging but is excellent at identifying bony involvement.
- MRI is far more sensitive and specific for local staging due to its superior delineation of the extent of involvement in lung tissue, surrounding blood vessels, spinal cord involvement, and brachial plexus invasion.
- Positron emission tomography-computed tomography (PET-CT) is useful in assessing nodal and distal metastasis, and accurate delineation of gross tumor volume at baseline staging; this is helpful for radiation treatment planning.
- Chest CT and PET-CT scans are considered mandatory before and after preoperative therapy, but recommendations vary on whether mediastinoscopy or endobronchial/esophageal ultrasound is necessary.
- Needle biopsy to check the tissue characteristics may help determine the type of cancer cells. [3]
How is PT treated?
The Standard of care is currently chemoradiation therapy to shrink the size of the tumor, followed by surgical resection. Induction chemotherapy includes combination chemotherapeutic drugs like cisplatin/etoposide or cisplatin/mitomycin, or cisplatin/vindesine.
Contraindications to surgery include:
- Involvement of intervertebral foramina or >50% vertebral bodies.
- Involvement of soft tissue at the base of the neck, e.g., esophagus or trachea.
- Mediastinal perinodal or contralateral supraclavicular nodal involvement.
- Venous obstruction.
- Presence of metastases.
Extensive invasion of the brachial plexus, especially above the T1 nerve root.
In some cases, surgeons may use a combination of surgery and chemoimmunotherapy (a combination of chemotherapy and immunotherapy).
When surgery isn`t an option, your oncologist may recommend having a combination of chemoradiation and immunotherapy or stand-alone radiation therapy to slow cancer growth. [2]