Opportunistic Bilateral Salpingectomy and Ovarian Cancer Prevention: What New Research Reveals
Ovarian cancer remains one of the deadliest gynecologic cancers worldwide. Despite advances in treatment, long term survival rates have remained stubbornly low, largely because the disease is often diagnosed at an advanced stage. New evidence published in JAMA Network Open in February 2026 adds to a growing body of research suggesting that opportunistic bilateral salpingectomy may significantly reduce the risk of the most common and aggressive form of ovarian cancer.
This article breaks down the latest findings, explains what opportunistic bilateral salpingectomy is, and explores what these results could mean for ovarian cancer prevention strategies in the future.
Understanding Ovarian Cancer and Why Prevention Matters
Ovarian carcinoma is not a single disease. It is a heterogeneous group of cancers with distinct biological behaviors and risk profiles. Among these, high grade serous carcinoma accounts for roughly 70 percent of all ovarian cancer cases and is responsible for the majority of ovarian cancer related deaths.
The five year survival rate for ovarian cancer remains below 50 percent. One major reason is that early stage ovarian cancer rarely causes noticeable symptoms. As a result, many patients are diagnosed only after the cancer has spread beyond the ovaries.
Because effective screening tools for ovarian cancer are still lacking, prevention has become a critical area of focus. Researchers and clinicians have increasingly turned their attention to the fallopian tubes as a key site of origin for high grade serous carcinoma.
What Is Opportunistic Bilateral Salpingectomy?
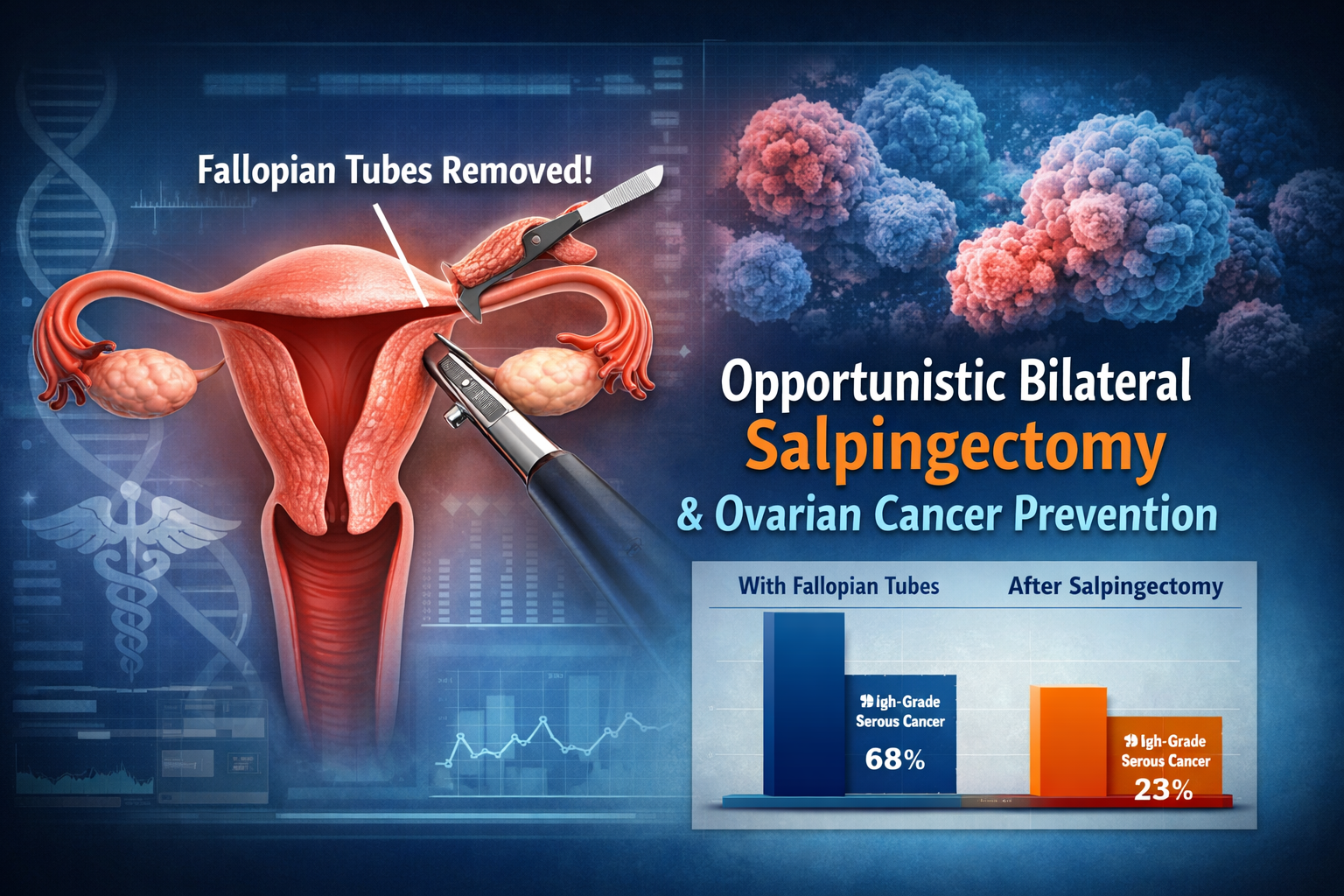
Opportunistic bilateral salpingectomy, often abbreviated as OBS, refers to the surgical removal of both fallopian tubes during another planned pelvic surgery. Common situations include hysterectomy for benign conditions or permanent contraception procedures.
Importantly, the ovaries are left intact. This distinction matters because the ovaries play a crucial role in hormone production. Preserving them helps avoid early menopause and its associated risks, such as cardiovascular disease and osteoporosis.
Previous studies have shown that OBS is safe, does not appear to accelerate the onset of menopause, and is cost effective when performed during already indicated surgeries. The new research expands on this evidence by directly examining cancer outcomes.
Overview of the JAMA Network Open Study
The research letter titled Serous Ovarian Cancer Following Opportunistic Bilateral Salpingectomy was published online on February 2, 2026 in JAMA Network Open. The study was conducted by a large international team of researchers led by investigators from the University of British Columbia.
The study had two primary objectives. First, to estimate the reduction in risk of serous ovarian cancer among individuals who underwent OBS compared with those who had other gynecologic surgeries. Second, to evaluate whether the types of ovarian cancer diagnosed in people without fallopian tubes differed from historical patterns.
Study Design and Methods Explained Simply
For the first objective, researchers conducted a population based retrospective cohort study in British Columbia. The study included all individuals who underwent hysterectomy or tubal permanent contraception between 2008 and 2020.
Participants were divided into two groups. One group underwent opportunistic bilateral salpingectomy. The comparison group underwent hysterectomy alone or tubal ligation without removal of the fallopian tubes.
Researchers followed participants over time and used statistical models to compare the risk of developing serous ovarian cancer between the two groups. Because most serous ovarian cancers are high grade, low grade and high grade serous carcinomas were combined in the analysis.
To assess whether differences between the groups could be due to selection bias, the researchers also analyzed breast cancer risk as a control outcome.
For the second objective, pathologists from multiple countries contributed anonymized data on ovarian cancer cases that occurred in individuals who no longer had fallopian tubes. The distribution of cancer subtypes in this group was compared with historical data using established statistical tests.
Key Findings From the Study
The results were striking.
Among more than 85,000 individuals included in the population based analysis, those who underwent opportunistic bilateral salpingectomy had a substantially lower risk of developing serous ovarian cancer. The crude hazard ratio was 0.22, meaning an estimated risk reduction of nearly 80 percent compared with the comparison group.
In contrast, there was no meaningful difference in breast cancer risk between the two groups. This finding strengthens confidence that the reduced ovarian cancer risk was not simply due to healthier individuals choosing OBS.
The second part of the study revealed an equally important insight. Among ovarian cancer cases diagnosed in individuals without fallopian tubes, only 23 percent were high grade serous carcinomas. Historically, this subtype accounts for more than two thirds of ovarian cancer cases.
This dramatic shift in cancer subtype distribution supports the theory that many high grade serous cancers originate in the fallopian tubes rather than the ovaries themselves.
Why These Findings Matter
This study provides some of the strongest real world evidence to date that opportunistic bilateral salpingectomy can meaningfully reduce the risk of the deadliest form of ovarian cancer.
Rather than relying on screening methods that have not proven effective, OBS represents a primary prevention strategy. It targets the tissue where many cancers appear to begin, while preserving ovarian function.
From a public health perspective, the implications are significant. Even a modest increase in the routine use of OBS during gynecologic surgeries could translate into fewer ovarian cancer diagnoses and deaths over time.
Addressing Safety and Limitations
While the results are compelling, the authors note several limitations.
Many of the individuals who underwent OBS were younger than the typical age at which high grade serous carcinoma is diagnosed. As a result, the total number of ovarian cancer cases observed during follow up was relatively small. This limited the ability to adjust for all potential confounding factors.
Despite this, the consistency of the findings across different analyses and the biological plausibility of the results lend credibility to the conclusions.
Importantly, prior research has shown that OBS does not significantly affect ovarian blood supply or hasten menopause. This addresses one of the most common concerns raised by patients and clinicians.
Implications for Patients and Clinicians
For individuals already planning gynecologic surgery for benign reasons, these findings support discussing opportunistic bilateral salpingectomy as part of informed consent.
For clinicians, the study reinforces existing recommendations in several countries that encourage OBS during hysterectomy or permanent contraception procedures when appropriate.
However, OBS is not a blanket recommendation for everyone. Decisions should be individualized, taking into account a patient’s age, reproductive plans, overall health, and personal values.
The Future of Ovarian Cancer Prevention
The growing body of evidence supporting opportunistic bilateral salpingectomy marks a shift in how ovarian cancer prevention is approached.
Instead of focusing solely on high risk populations or genetic predisposition, OBS offers a population level intervention that can be integrated into standard surgical care.
Ongoing research will be needed to confirm long term outcomes as the cohort ages and to explore how OBS might interact with other risk factors. Still, the current data suggest that this strategy holds real promise.
Final Thoughts
Ovarian cancer has long been a disease where prevention options were limited and early detection remained elusive. This new research published in JAMA Network Open provides strong evidence that removing the fallopian tubes during routine gynecologic surgery can substantially reduce the risk of the most lethal ovarian cancer subtype.
As awareness grows and guidelines continue to evolve, opportunistic bilateral salpingectomy may become a cornerstone of ovarian cancer prevention.
Source
Sowamber R, Mei AJ, Kaur P, et al. Serous Ovarian Cancer Following Opportunistic Bilateral Salpingectomy. JAMA Network Open. Published February 2, 2026. 2026;9(2):e2557267. doi:10.1001/jamanetworkopen.2025.57267
Disclaimer
This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Clinical decisions should always be made in consultation with a qualified healthcare professional, taking into account individual patient circumstances. All interpretations are based on the cited study and do not necessarily reflect the views of medical institutions, clinicians, or regulatory bodies.