Core Stability – A Concept
What is core stability?
The term core refers to the lumbo–pelvic–hip complex, where the center of gravity is located. The muscles that make up this complex provide a stable base from which the extremities work. The term core strength refers to the strength and endurance of the muscles of the lumbo–pelvic–hip complex, whereas stability refers to the ability to use strength and endurance in a functional manner. Function is defined as a multiplanar movement that involves acceleration, deceleration, and stabilization. To be mechanically efficient, athletes must combine strength and stability training in their reconditioning programs. Core strength and stability together is called functional strength. Functional strength is the ability to produce concentric acceleration force, isometric stabilization force, and eccentric deceleration force in all three planes of movement during activity.
The central nervous system plays an integral role in core stability. This system controls proprioception, which is the interpretation of sensory information and the response to position sense. Receptors in the skin, joints, muscles, and tendons send information to the central nervous system, which, in turn, sends appropriate information back to the muscles to provide neuromuscular control. In other words, core stability is the ability of the central nervous system to interpret the position of the body in space and to react accordingly. Appropriate muscle strength is needed to support the spine and to dynamically stabilize the body. With injury or a lack of training, proprioception can be altered, thus emphasizing the need for stabilization exercises. (https://www.sciencedirect.com/science/article/abs/pii/B9781416031970100357)
Core stability refers to the body's ability to resist opposing forces that may affect spinal control (Akuthota et al., 2008). The term ‘core’ should be thought of an inclusive descriptor of all the musculature and soft tissues that protects and stabilizes the spine, and pelvis and regulates postural stability (Panjabi, 2003). The concept of core strengthening was proposed in the later part of the 1990's (Lederman, 2010) and has been used to describe lumbar stabilization, motor control training, and other specific regimens (Akuthota et al., 2008; Standaert and Herring, 2007). Ever since its inception, it has been a salient concept both in clinical rehabilitation and competitive athletic training (Clark et al., 2018). Core stabilization is therefore a fundamental part of low back pain rehabilitation. (https://www.sciencedirect.com/topics/medicine-and-dentistry/core-stability)
Lumbar stabilization is the natural ability of the spinal column to maintain its anatomical structure on physiological loading. The stability is maintained by the interaction between the bony structure with ligaments, the attached muscles, and the nervous system that connects the above two. Natural disc degeneration combined with sedentary behavior can lead to weakness of the muscles, which can then cause segmental instability. Back pain is the largest cause of disability-adjusted living years based on the WHO survey of the global burden of disease.
What are the factors responsible to maintain spinal stability?
In the 1990s, Manohar Panjabi postulated that the following three interacting systems were responsible for the maintenance of spinal stability:
- The active system comprising of the muscles and
- The neural system that interacts between these two systems.
The passive system comprising of the vertebral bodies, the intervertebral discs, the zygapophyseal joints, the zygapophyseal joint capsules, and the spinal ligaments.

In a normal healthy spine, the above three systems interact and allow normal function and pain-free range of movement (ROM). With stress loading of the passive system (vertebrae, disc, ligaments, and joints), the active system (muscles) come into play and prevent abnormal deformation. The contribution of the passive system in the neutral spine is minimal. Cadaveric experiments show that when the muscles are removed, and only the bones, discs, and the ligaments are left in situ, the spine buckles under low loads of 20 lbs (9 kg).
The neural control subsystem receives input both from the passive and the active subsystems and then direct the spinal musculature to stabilize the spine. The neural system should act at the right time and the right amount to protect the spine from injury and to allow the desired movement.
An inability of the active system to maintain the relationship between different elements of the passive system during physiological loading can lead to spinal pain. Based on this, clinical instability can be defined as the abnormal displacement that occurs within the motion segment when a normal physiological load is applied. In a healthy state, if the three systems interact and provide stability, then following injury or degeneration to the passive system, the active system needs to work harder to compensate for the decreased contribution from the passive system.

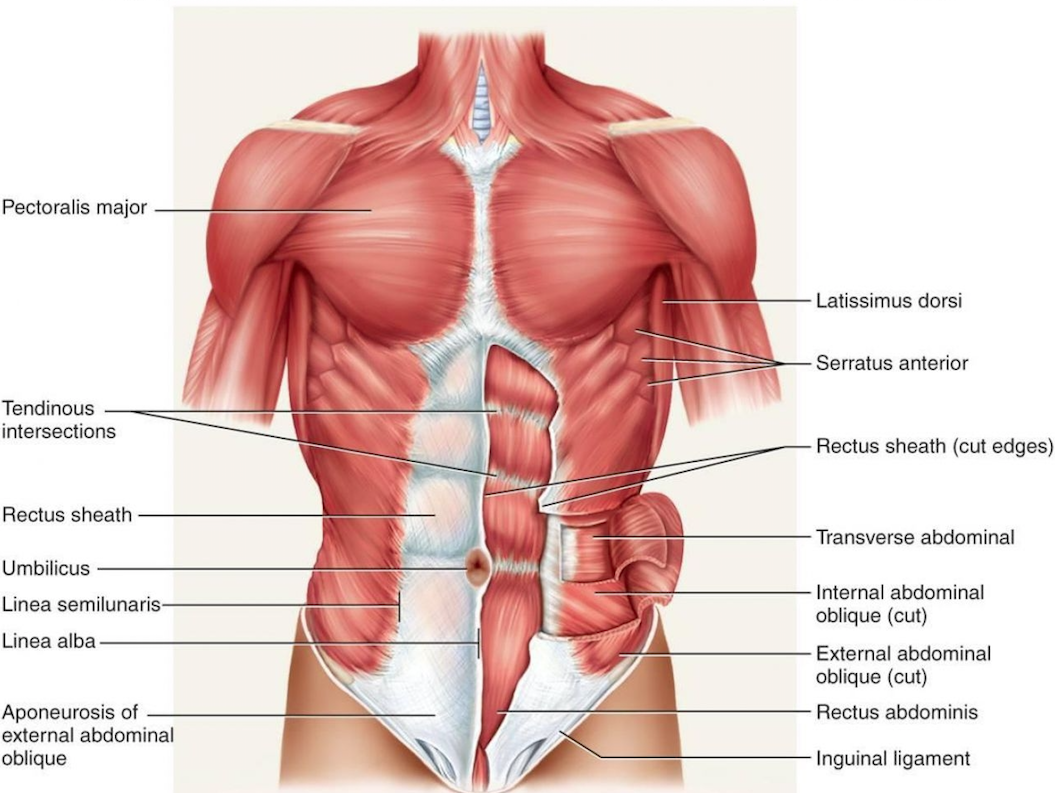
Which muscles comprise the core?
The core can be described as a muscular box with the abdominals in the front, paraspinals and gluteals in the back, the diaphragm as the roof, and the pelvic floor and hip girdle musculature as the bottom. Within this box are 29 pairs of muscles that help to stabilize the spine, pelvis, and kinetic chain during functional movements. Without these muscles, the spine would become mechanically unstable with compressive forces as little as 90 N, a load much less than the weight of the upper body. When the system works as it should, the result is proper force distribution and maximum force generation with minimal compressive, translational, or shearing forces at the joints of the kinetic chain. (https://journals.lww.com/acsm-csmr/Fulltext/2008/01000/Core_Stability_Exercise_Principles.14.aspx)
(Source: Richardson, C., G. Jull, P. Hodges, and J. Hides. Therapeutic exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach. Edinburgh, NY: Churchill Livingstone, 1999.)