Bronchiectasis: Causes, Symptoms, Diagnosis, and Treatment
Bronchiectasis is a chronic lung disease that usually begins with injury to the walls of the airways from an infection or other conditions. It leads to weakening of the mucociliary transport mechanism, owing to repeated infection, contributing to bacterial invasion and mucus pooling throughout the bronchial tree. Over time, the airways become stretched out, flabby, scarred, and unable to move air in and out. Bronchiectasis usually begins in childhood, but symptoms may not appear until months or even years after you have started having repeated lung infections.
How common is bronchiectasis?
Bronchiectasis affects 350,000 to 500,000 adults in the United States. The risk of developing bronchiectasis increases with age.
What causes bronchiectasis?
The majority of bronchiectasis cases are triggered by the following underlying conditions:
- Cystic fibrosis
- Autoimmune disease
- Immunodeficiency disorders, such as HIV or diabetes
- Chronic obstructive pulmonary disease (COPD) and alpha-1-antitrypsin deficiency, which can cause COPD in some people
- Diseases that affect the cilia, the small, hair-like structures that line your airways, and whose main function is to clear mucus
- Inflammatory bowel disease, including Crohn’s and ulcerative colitis
- Allergic bronchopulmonary aspergillosis, which is a type of allergic lung inflammation of the airways
- Chronic pulmonary aspiration, problems with swallowing that cause food or fluids to get into the lungs, and lead to inflamed airways
- Infections such as pneumonia
- Pertussis (whooping cough)
- Tuberculosis
- Other viral or fungal infections
- Bronchial obstruction caused by foreign bodies, mucus, or tumors
- Hilar lymphadenopathy
What are the symptoms of bronchiectasis?
Mild to moderate bronchiectasis may present with:
- Daily cough, for months or years
- Daily production of large amounts of mucus, or phlegm
- Repeated lung infections
- Shortness of breath
- Wheezing
- Chest pain
Over time, more serious symptoms may develop, including:
- Coughing up blood or bloody mucus
- Weight loss
- Fatigue
- Sinus drainage
Bronchiectasis can also lead to other serious health conditions, including collapsed lung, heart failure, and brain abscess.
How is bronchiectasis diagnosed?
Your doctor will ask you about your history of symptoms and other illnesses and listen to your lungs to test how well they’re working. To confirm the diagnosis of bronchiectasis, the following tests can be ordered:
- Chest CT scan or a chest X-ray
- Blood tests and sputum cultures to find infections
- Lung function test, such as spirometry
- Genetic testing to detect autoimmune or alpha-1-antitrypsin deficiency
- Sweat chloride test to find if you have cystic fibrosis
- Bronchoscopy to find and remove anything blocking your airways and get samples of mucus or pus from your lungs for testing.
What is the treatment for bronchiectasis?
- Treating the underlying cause of bronchiectasis, such as immunoglobulin replacement, steroids, treatment for nontuberculous mycobacteria, and Cystic fibrosis.
- Improving tracheobronchial clearance by way of postural drainage. Most physicians recommend mucus clearance as the mainstay of therapy in bronchiectasis. It is recommended to be performed for a minimum of 5 to 10 minutes twice a day. Efficiently performed, this is of great value both in reducing the amount of cough and sputum and in preventing recurrent episodes of bronchopulmonary infection.
- A physical therapist can teach the active cycle of breathing technique, which helps direct secretions in the dilated bronchi to gravitate towards the trachea, from which vigorous coughing can clear them. "Percussion" of the chest wall with cupped hands may help to dislodge sputum, and a number of mechanical devices are available, which cause the chest wall to oscillate, thus achieving the same effect.
- Infection control is based on the results of culture and sensitivity. When no specific pathogen is identified, and the patient is not seriously ill, an oral agent like amoxicillin, co-amoxiclav, or macrolides for 2 weeks is sufficient.
- Higher dose of oral amoxicillin 1 gm twice per day for 2 weeks, especially if colonized with H. influenza.
- If pseudomonas-colonized, then a 2-week course of ciprofloxacin 750 mg twice per day (with cautious use in the elderly) is reasonable.
- For moderate-to-severe symptoms, parenteral antibiotics, such as an aminoglycoside (gentamicin, tobramycin), antipseudomonal synthetic penicillin, a third-generation cephalosporin, or a fluoroquinolone, may be indicated.
- Control reverse airflow obstruction with inhaled bronchodilators and corticosteroids.
- As with other respiratory diseases, patients with bronchiectasis should be encouraged to stop smoking. Vaccination against influenza and pneumococcal disease is also recommended.
Treatment for Pseudomonas isolates includes 2 weeks of intravenous (IV) antipseudomonal antibiotics, nebulized colistin for 3 months, or nebulized colistin for 3 months with an additional 4 weeks of oral ciprofloxacin.
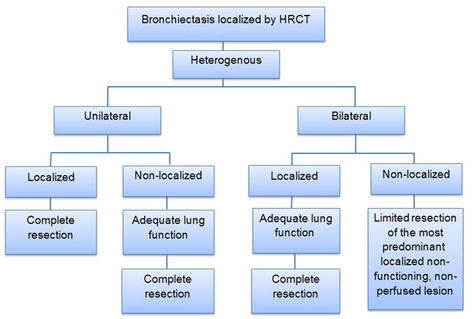
What are the surgical options to treat bronchiectasis?
Surgery can help only a small proportion of cases, for e.g., young patients in whom the bronchiectasis is unilateral and confined to a single lobe or segment, as demonstrated by CT. Surgery may also be first-line treatment for the management of massive haemoptysis.
Single- or double-lung transplantation has been used as a treatment of severe bronchiectasis, predominantly when related to Cystic fibrosis. In general, consider patients with Cystic fibrosis and bronchiectasis for lung transplantation when FEV falls below 30% of the predicted value.