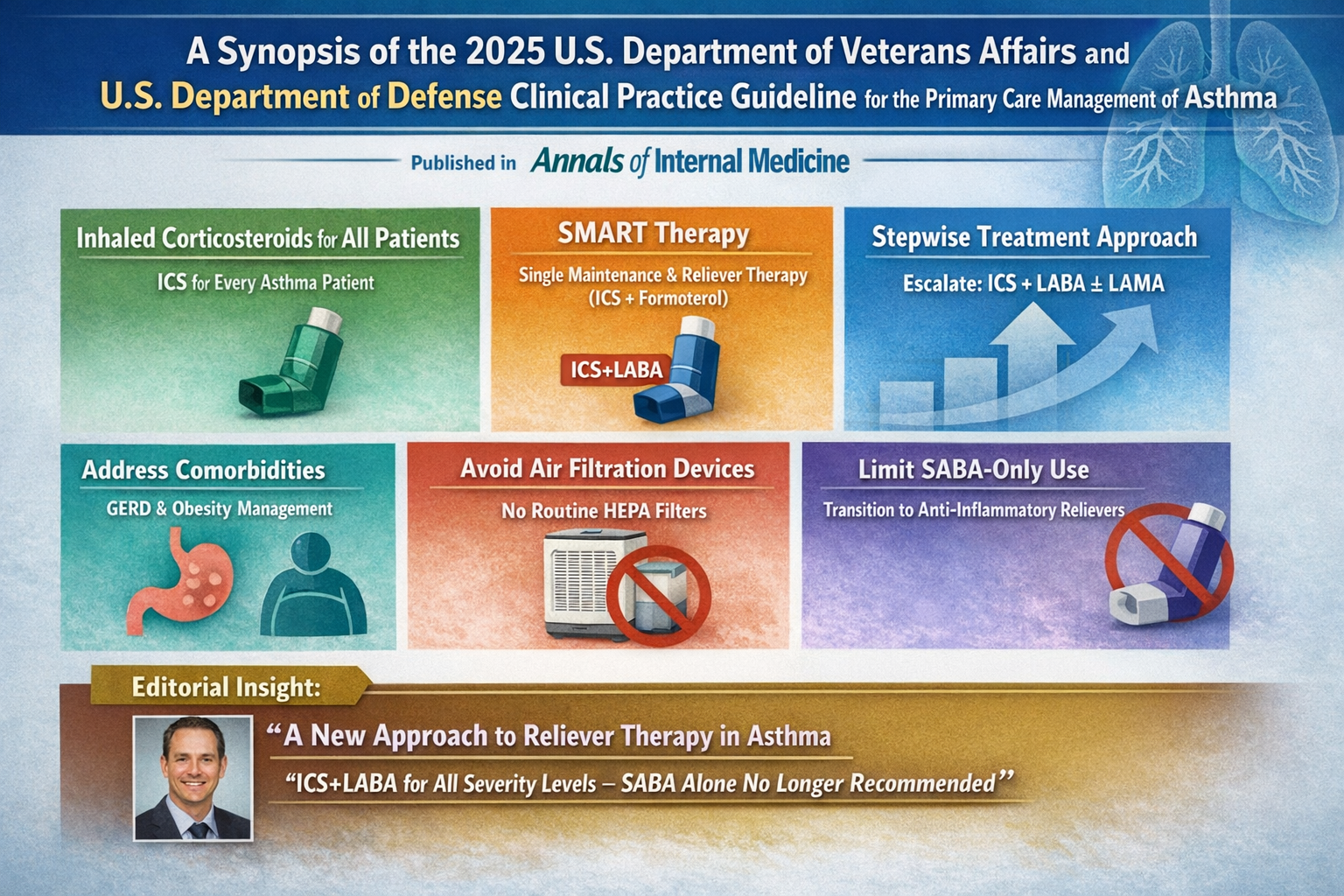
A Synopsis of the 2025 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline for the Primary Care Management of Asthma
Asthma remains one of the most common chronic respiratory diseases managed in primary care. In 2025, the U.S. Department of Veterans Affairs and the U.S. Department of Defense released an updated joint clinical practice guideline that significantly reshapes chronic asthma management in outpatient settings.
Published in Annals of Internal Medicine, the updated guideline reflects evolving evidence on inhaled corticosteroids, reliever therapy strategies, and comorbidity management. This SEO optimized blog provides a detailed synopsis of the 2025 VA DOD Clinical Practice Guideline for the primary care management of asthma, along with insights from a related 2026 editorial that further clarifies the clinical implications of these changes.
Background: Why the 2025 VA DOD Asthma Guideline Is Important
Asthma affects nearly 25 million people in the United States and approximately 8.7 percent of U.S. adults. It disproportionately impacts women, older adults, individuals with obesity, and people with lower household income. These demographics are well represented within VA and DOD health systems.
Despite advances in pharmacotherapy, more than half of patients with asthma remain uncontrolled. Many experience recurrent exacerbations that are preventable with optimized treatment strategies. Historically, asthma care relied heavily on short acting beta agonist relievers combined with maintenance inhaled corticosteroids. However, real world adherence to daily ICS therapy has been inconsistent.
The 2025 VA DOD guideline addresses this gap by prioritizing anti inflammatory reliever strategies and simplifying treatment frameworks for primary care clinicians.
How the Guideline Was Developed
The guideline work group followed standards set by the National Academy of Medicine for trustworthy clinical practice guidelines. Literature published between July 20, 2018 and May 15, 2024 was systematically reviewed.
Using the GRADE framework, recommendations were based on:
- Quality of evidence
- Balance of benefits and harms
- Patient values and preferences
- Feasibility and resource considerations
Fifty nine studies informed 21 evidence based recommendations. The guideline focuses specifically on chronic asthma management in primary care for patients older than 5 years. Acute exacerbation management and biologic therapies were intentionally excluded.
Major Shift: Inhaled Corticosteroids for All Patients
One of the strongest messages from the 2025 VA DOD asthma guideline is the universal recommendation for inhaled corticosteroids.
Strong Recommendation
All patients with asthma should receive ICS therapy, regardless of symptom frequency or historical severity classification.
This marks a shift from previous approaches that reserved ICS primarily for persistent asthma. Evidence now demonstrates that even patients with infrequent symptoms remain at risk for severe exacerbations. Inflammation control must be foundational in asthma management.
The Rise of SMART and MART Therapy
A defining feature of the updated guideline is support for single maintenance and reliever therapy, commonly referred to as SMART or MART.
What Is SMART?
SMART uses a single inhaler that contains:
- An inhaled corticosteroid
- A rapid onset long acting beta agonist, typically formoterol
The inhaler is used for both daily maintenance and symptom relief.
The guideline suggests ICS combined with rapid onset LABA as both controller and reliever therapy in patients aged 12 years and older.
Evidence Behind SMART
Randomized trials involving approximately 22,000 participants show that SMART reduces severe exacerbations by about one third compared with traditional maintenance plus short acting reliever approaches.
By delivering anti inflammatory therapy during symptomatic periods, SMART addresses the problem of over reliance on rescue inhalers and underuse of maintenance ICS.
Stepwise Asthma Treatment Framework
The 2025 VA DOD guideline retains a stepwise treatment model while redefining escalation strategies.
Step Up From ICS Alone
For patients uncontrolled on ICS alone, the guideline strongly recommends transitioning to ICS plus rapid onset LABA as both controller and reliever.
Systematic reviews demonstrate that this strategy reduces exacerbation frequency and severity compared with increasing ICS dose alone or adding leukotriene receptor antagonists.
Triple Therapy
If asthma remains uncontrolled on moderate or high dose ICS plus LABA, the guideline suggests adding a long acting muscarinic antagonist.
Evidence from large randomized trials supports improved symptom control and reduced moderate to severe exacerbations with triple therapy.
Step Down Therapy
For patients whose asthma has been controlled for at least three months, clinicians should consider step down therapy to minimize adverse effects while maintaining control.
Complete discontinuation of ICS is not recommended. Instead, clinicians may reduce ICS dose or discontinue LABA while continuing some level of anti inflammatory therapy.
Addressing Comorbid Conditions
Gastroesophageal Reflux Disease
The guideline suggests treating symptomatic gastroesophageal reflux disease in patients with asthma and GERD. A systematic review of 23 randomized controlled trials found improved asthma control and lung function with GERD treatment.
Obesity and Weight Management
Weight loss is recommended for adults with asthma and obesity. Studies show that losing more than 5 percent of body weight results in meaningful improvements in patient reported asthma control.
Recommendation Against Indoor Air Filtration Devices
The work group suggests against routine use of indoor air filtration devices such as high efficiency particulate air filters.
Multiple studies showed no clinically significant improvements in asthma control, exacerbations, or lung function. Financial costs to patients further limit their value in routine primary care management.
Monitoring and Follow Up
The guideline suggests against routine spirometry for stable asthma monitoring in primary care. Spirometry remains useful for diagnosis and selected cases but is not required at every visit.
There is insufficient evidence to recommend for or against routine fractional exhaled nitric oxide testing or telemedicine as a replacement for in person visits.
Electronic health record tools such as reminders and tracking systems are encouraged to support adherence and monitoring.
Editorial Perspective: A New Approach to Reliever Therapy in Asthma
An accompanying editorial published on February 17, 2026 in Annals of Internal Medicine provides additional perspective on the guideline. Titled A New Approach to Reliever Therapy in Asthma: Implications of the U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline, the editorial was authored by James G. Krings, MD, MSc.
The editorial emphasizes that more than half of patients with asthma have uncontrolled disease, often due to reliance on short acting beta agonist inhalers without adequate anti inflammatory therapy.
Historically, patients were prescribed separate maintenance ICS inhalers and SABA relievers. Many patients prioritized immediate symptom relief and underused daily ICS therapy, leading to persistent airway inflammation. Observational studies link high SABA use and low ICS exposure to increased asthma related morbidity and mortality.
Over the past two decades, research has focused on coupling ICS delivery with reliever use. SMART therapy, often implemented with budesonide formoterol combinations, operationalized this concept. Across large trials, SMART reduced severe exacerbations by approximately one third.
The editorial highlights that the VA DOD guideline strongly recommends ICS containing reliever therapy across all levels of asthma severity. SABA only reliever therapy is no longer recommended.
Alignment With Global Guidelines
The editorial also situates the VA DOD update within broader international shifts.
In 2019, the Global Initiative for Asthma moved away from recommending SABA only treatment. Around the same time, the National Asthma Education and Prevention Program endorsed SMART for moderate to severe asthma but retained SABA only therapy for milder disease.
The VA DOD guideline represents one of the clearest U.S. endorsements of ICS containing reliever therapy across the full asthma severity spectrum.
Implementation Challenges
The editorial notes that adoption may be uneven due to formulary limitations and insurance coverage. Only certain LABA agents, such as formoterol, have rapid onset suitable for reliever use. Insurance coverage constraints may limit access to optimal inhalers.
When ICS formoterol inhalers are unavailable, fixed dose budesonide albuterol combinations may serve as alternative anti inflammatory reliever options, although evidence is less robust and costs may be higher.
Health systems are encouraged to align formularies with contemporary evidence to improve outcomes and reduce inequities.
Public Health and Equity Considerations
Between 1986 and 2020, the U.S. Food and Drug Administration approved more than 60 inhalers for asthma and chronic obstructive pulmonary disease. Despite expanded options, asthma related morbidity and mortality have improved only modestly.
Disease burden remains concentrated in lower socioeconomic and lower health literacy populations. These groups are more likely to rely on SABA only therapy and less likely to receive adequate ICS exposure.
Coupling reliever use with anti inflammatory therapy may reduce disparities while improving outcomes.
Key Clinical Takeaways
For primary care providers, the 2025 VA DOD asthma guideline and accompanying editorial reinforce several core principles:
- Prescribe inhaled corticosteroids for all patients with asthma.
- Prefer ICS plus rapid onset LABA as controller and reliever therapy for patients aged 12 and older.
- Escalate to triple therapy when necessary.
- Address comorbid GERD and obesity.
- Avoid routine indoor air filtration devices.
- Transition patients away from SABA only regimens.
- Refer complex cases and biologic candidates to specialists.
The central theme is clear: integrate anti inflammatory therapy into every stage of asthma care.
Conclusion
The 2025 VA DOD Clinical Practice Guideline for the primary care management of asthma represents a decisive shift toward inflammation centered, simplified treatment strategies. Strong endorsement of inhaled corticosteroids and SMART based therapy reflects a mature evidence base demonstrating reduced exacerbations and improved outcomes.
Combined with insights from the 2026 editorial in Annals of Internal Medicine, the message to clinicians is direct. Replace SABA only strategies with ICS containing reliever therapy wherever feasible. Align everyday practice with contemporary evidence. Simplify regimens to improve adherence. Address comorbid conditions and health system barriers.
For millions of patients with asthma managed in primary care, these changes offer a meaningful opportunity to reduce preventable exacerbations and improve long term respiratory health.
Sources
Sharafkhaneh A, Atayde ER, Cho J, et al. A Synopsis of the 2025 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline for the Primary Care Management of Asthma. Annals of Internal Medicine. 2026.
Krings JG. A New Approach to Reliever Therapy in Asthma: Implications of the U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline. Annals of Internal Medicine. 17 February 2026. DOI:
Disclaimer
This article is for informational and educational purposes only and summarizes published clinical practice guidelines and editorial commentary. It does not constitute medical advice. Clinicians should consult the full guideline documents and exercise independent clinical judgment. Patients should seek evaluation and treatment from qualified health care professionals for asthma or any other medical condition.